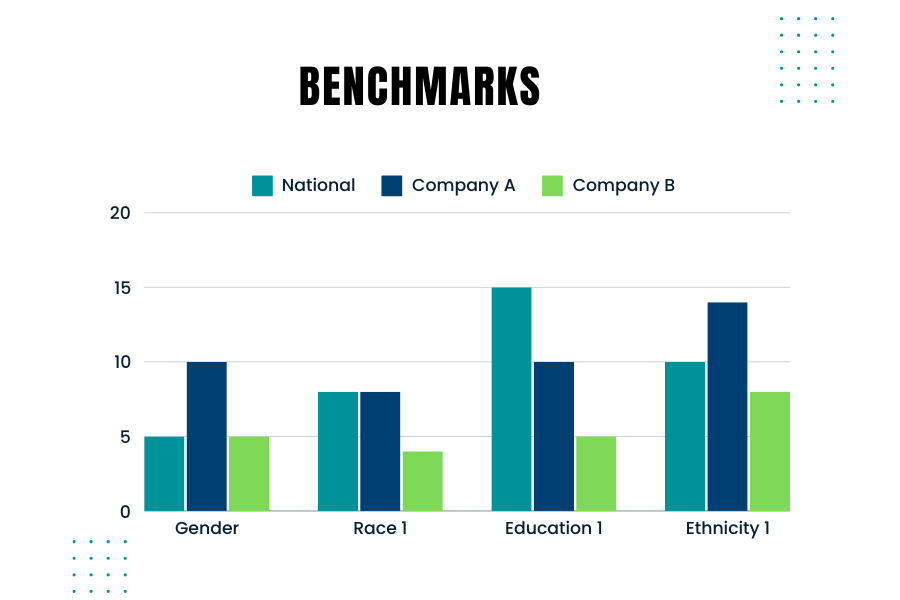
Creating and using benchmarks to compare your company’s hiring demographics against those used by government agencies like the EEOC (Equal Employment Opportunity Commission) is crucial. Benchmarking helps ensure that your company’s hiring practices are fair and compliant with federal regulations. Here’s are some considerations to keep in mind when you consider the right benchmarks
Why Benchmarking Matters
Government agencies monitor and require companies to report on the demographic composition of their workforce, especially larger companies. For instance, the EEOC uses benchmarks to compare a company’s demographics against broader population data from sources like the U.S. Census and the American Community Survey. Knowing how your company’s demographics stack up against these benchmarks is essential for several reasons:
Diversity Goals: Meeting your company’s diversity and inclusion goals.
Fair Hiring Practices: Ensuring fair and unbiased hiring practices.
Best Practices for Benchmarking
Collect Internal Data: Gather detailed demographic data of your current workforce and applicants.
Ensure you track data on race, gender, age, and other relevant demographics.
Choose the Right External Data: Depending on your hiring scope, use national, regional, or local data. For example, if you recruit nationwide, use national benchmarks. For local hires, consider regional data.
Occupation and Industry-Specific Data: Align your benchmarks with the specific occupations and industries relevant to your company. Different industries and roles may have distinct demographic compositions.
Adjust for Educational Requirements: Consider the educational requirements for the roles you are hiring. This will help you compare your applicant pool against the qualified population.
Use Census Data: The U.S. Census Bureau provides comprehensive data that can be segmented by occupation, geography, and other factors. This data is a good starting point for creating your benchmarks.
Ensuring Fair Selection
To avoid over- or under-selecting any protected group, follow these steps:
Regularly Update Benchmarks: Demographic data changes over time. Ensure your benchmarks are based on the most recent data.
Monitor Hiring Practices: Continuously monitor your hiring practices and outcomes against your benchmarks.
Training and Awareness: Educate hiring managers on the importance of diversity and compliance with hiring practices.
External Data Sources
Looking at external data sources is important because it provides a broader context for your internal data. It helps you understand the labor market and demographic trends in your industry and location. External benchmarks serve as a snapshot of the current workforce composition, which can change over time.
Creating effective benchmarks involves a blend of using accurate external data and understanding your company’s unique needs. By comparing your company’s demographics against reliable benchmarks, you can ensure fair and compliant hiring practices. Regularly updating these benchmarks and educating your hiring team on best practices will help maintain a diverse and inclusive workforce.
Where Can You Find Additional Information?
Of Significance: Don’t Miss the Mark! Podcast on what to keep in mind when creating benchmarks
Harvard Business Review: Smart benchmarking starts with knowing whom to compare yourself to
The hospice Special Focus Program (SFP) is conducted by the Center for Medicare and Medicaid Services (CMS). The objective of this program is to identify poor performing hospice agencies, based upon quality indicators, that place hospice beneficiaries at risk. These hospice agencies will then be subject to additional scrutiny and oversight to ensure that they meet Medicare requirements. The SFP is designed to either bring these programs into compliance or force them out of the Medicare program by terminating their Medicare status.
What is the origin of the Special Focus Program?
The hospice Special Focus Program was mandated in the Consolidated Appropriations Act of 2021. That is also when it was clarified that hospices would be surveyed every three years. All hospices now have had a survey since 2021. Some of that data is being used for the hospice Special Focus Program, which is designed to identify the worst performing hospices and either bring them into compliance or force them out of the program by terminating their Medicare status.
How is a hospice agency selected for inclusion in the Special Focus Program?
CMS uses an algorithm to identify the poor performing hospice agencies to include in the SFP. The algorithm combines data from a few data sources to score each of the hospice agencies. The score is based on data from: condition-level deficiencies in standard surveys, substantiated complaints, Hospice Care Index (HCI), and the CAHPS survey. The algorithm does not stratify hospice agency based upon size or location; all hospice agencies are held to the same standard regardless of their size or location. The bottom 10% ranked hospice agencies (which are the hospice agencies with the highest algorithm score) are selected to be included in to the SFP.
What is the impact of a hospice agency being included in the SFP?
Hospice agencies that are included in the SFP will be publicly reported on the SFP website. SFP is a framework for increased oversight. The hospice agencies that are included in the SFP program will be surveyed more frequently — at least every six months. CMS will determine what actions must be taken based upon the survey results.
How will a hospice agency exit the SFP?
A hospice will complete the SFP if in an 18-month time frame the hospice agency has no Quality of Care condition level deficiencies or immediate jeopardies for any two six month SFP surveys and has no pending complaints or have returned to substantial compliance with all requirements. The hospice will receive a letter from CMS that will indicate official completion of the program. If a hospice is unable to meet the completion criteria – due to inability to successfully pass surveys or continued complaints while on the SFP – it will be placed on the Medicare termination track.
Even as hospices work to improve their levels of quality and compliance, there will always be hospice agencies that fall in the lowest 10% of performance relative to their peers. Only by continually monitoring their quality performance and comparing these quality scores to peer performance can a hospice agency stay out of the lower 10% and off of the SFP list.
In accordance with the Conditions of Participation, a Medicare certified hospice agency must have a governing body. The governing body has ultimate responsibility for the hospice agency, including legal and financial authority. Medicare Conditions of Participation require that the governing body is informed of the ongoing activities at the hospice agency, including patient care delivery issues and all QAPI activities. The governing body must also appoint a qualified hospice administrator – a hospice employee with the necessary education and experience – who is responsible for hospice daily operations.
The governing body must meet at least quarterly and must maintain written minutes of its meetings.
There are two Conditions of Participation – 418.100 and 418.58 – that relate to the hospice governing body.
Condition of Participation 418.100
This Condition of Participation defines a standard that the governing body is responsible for management of the hospice agency, including its fiscal operations, provision of services, and continuous quality assessment and performance improvement (QAPI) efforts. The governing body also assumes full legal authority of all hospice operations. It further specifies that the governing body should appoint an administrator that reports to the governing body and who is responsible for hospice agency daily operations. The hospice administrator must be a hospice employee and must have necessary training, education, and experience. CMS does not specify the process by which an administrator should be selected by the governing body. If a hospice agency has multiple locations, the governing body is responsible for administration, supervision, and services for all locations as well as for any arranged services.
Condition of Participation 418.58
This Condition of Participation discusses requirements of a hospice agency’s QAPI program. The governing body must ensure that the hospice agency maintains and implements an ongoing quality improvement and patient safety program. Program performance must be monitored on a regular basis. Further, the governing body must ensure that one or more individuals are selected to lead the organization’s QAPI efforts.
The hospice agency’s organization documents must specify that the hospice governing body is responsible for the QAPI program. Additionally, the governing body specifies the frequency of data collection and level of detail of data collected by the QAPI program.
Are there any state regulations?
State hospice licensure regulations may impose additional requirements on the hospice governing body. They may also have specific requirements on the administrator that is selected by the governing body. A hospice is required to meet the most stringent requirements (whether state or federal).
Surveyors will check that all conditions are met. A hospice agency should maintain evidence of the governing body’s role and activities. Governing body authorizations and activities should be documented in governing body meeting minutes, company organization documents, and company policies and procedures.
Prior to the third hospice benefit period, and prior to each subsequent benefit period, a hospice physician or nurse practitioner is required to have a face to face encounter with the hospice patient to recertify that the patient continues to be Medicare eligible for hospice benefits. The face to face encounter must occur within 30 calendar days prior to the start of the third benefit period and each subsequent benefit period.
The face to face encounter is necessary to recertify that the patient remains eligible for Medicare hospice benefits. If face to face encounters are not performed timely, the patient is is no longer hospice eligible. The hospice may continue to provide hospice services to the patient but may no longer continue to bill Medicare. Instead, the hospice would need to assume all financial responsibility for the patient until such time that the hospice is able to reestablish patient hospice eligibility. The patient may be readmitted to hospice once hospice eligibility criteria are once again met.
What if there are exceptional circumstances that cause the hospice to be unable to timely complete the face to face encounter?
What are exceptional circumstances?
If a patient is admitted and is in the third benefit period or later, the hospice agency may be unable to perform the face to face encounter prior to the start of the benefit period.
For example, if the patient is an emergency weekend admission and the nurse practitioner or hospice physician is unable to meet with the patient prior to hospice admission. The patient is only seen the following Monday.
Another exceptional circumstance may be where the CMS data system is unavailable and the hospice agency is unaware that the patient is in the third or later benefit period.
In these documented exceptional circumstances, the face to face encounter is considered timely if it is completed within two days after admission.
In addition, if the patient dies within two days of admission, the face to face encounter is considered complete.
What is hospice initial accreditation and why is it important?
Hospice initial accreditation is a way to ensure delivery of consistent and high quality services across all accredited hospice agencies. The accreditation program ensures that the hospice agency is fully compliant with Medicare Conditions of Participation. The program also reviews that the hospice is compliant with state and local laws. An on-site survey conducted by the accrediting organization evaluates the quality of the clinical care provided, quality and compliance of patient records, policies and procedures, and performance improvement. Patient and family experiences and quality outcomes are also reviewed. The organization’s financial and long term viability is also studied via review of budgets and other related metrics.
When would a hospice want to complete the accreditation process?
A home hospice must complete the initial Medicare accreditation process before it is able to bill Medicare for services provided to patients. CMS has approved three accrediting organizations (AO) to conduct Medicare surveys and accreditation for hospice agencies: CHAP, ACHC, and JCAHO. These agencies have standardized accreditation and assessment processes although the requirements and actual on-site survey review may vary depending upon state and local regulations.
There are six key elements of the initial accreditation process
File and obtain state home licensure
Register with accreditation organization
Obtain CMS 855A
Develop patient caseload – verify agency is meeting Conditions of Participation
Ensure Conditions of Participation are being met
On-site survey visit
We now discuss each of these elements in greater detail.
Element 1: The process begins with the hospice filing a state home hospice licensure. Each state has its own requirements for approval. So this process and its time lines will differ by state.
Element 2: Register with one of the three accreditation organizations (AO). The AO will require a registration fee. Although the accreditation will be received from CMS, Medicare has granted authorization to AO to conduct the accreditation process on behalf of CMS. The AOs have local branches, allowing them to customize their surveys for state and local regulatory requirements.
Element 3: Confirm 855A is accepted by the Medicare Administrative Contractor (MAC) that is appropriate for the hospice agency’s region: Palmetto GBA, NGS or CGS.
Element 4: Develop patient caseload. Specifically, the hospice must have serviced five patients, with at least three active at the time that the AO conducts the survey. Further, although the hospice is not currently billing Medicare, all patients must be treated as if they are Medicare eligible. All documentation must be completed within the Medicare required time frames and services must be provided by employees, as per Medicare guidelines.
Element 5: Ensure Conditions of Participation are being met. This element involves a number of different items.
The first item is that the hospice agency must verify it is providing all core services using hospice agency employees. Core services include nursing, social work, and counseling including spiritual, bereavement, and dietician. These services must be provided using hospice employees. Contractors may not be used to provide these services. Physician is also a core service but CMS permits the medical director and alternate medical director services to be provided using either hospice agency employees or contracted services.
The second item is to very that the hospice agency is able to provide all non core services using either hospice agency employees or contractors. Non core services include the therapies: physical therapy, occupational therapy, and speech therapy. Additionally, the agency must verify that it is able to provide aide services. It also must be able to demonstrate that it has a bereavement program, even if this service is not yet being used.
The third element is that the hospice agency must verify it can provide all four levels of care including routine, GIP, respite, and continuous care. Not all of these levels of care must be provided through hospice employees; the agency may contract to provide these levels of care.
As a final element, the hospice agency should demonstrate that it can provide DME, pharmaceuticals, drugs and biologicals.
Element 6: On-site survey. Once the hospice confirms that that prior five elements are completed, it will indicate to the AO that it is ready for a Site Visit. The date of the Site Visit will not be announced to the hospice agency but will typically occur within 45 days of when the hospice agency indicates site readiness. The survey will be conducted on-site over three consecutive days. The AO will review patient medical records, accompany staff on patient home visits, and review both clinical and non-clinical hospice agency policies and procedures. The AO will also review the agency for financial viability by reviewing budgets and other related metrics.
What happens after the survey is completed?
After the AO completes the on-site survey, the hospice agency will be notified of the final findings of the survey. There are four possible outcomes.
Agency passed with no deficiencies
Agency passed with minor deficiencies; agency must write an action plan that must be accepted by the accrediting organization
Agency has major deficiencies; deficiencies must be resolved, followed by another three day survey
Agency failed the survey; agency must restart the entire process
What happens after a hospice agency is issued its accreditation letter?
The AO sends a copy of the accreditation letter to the state department of health. Upon receipt, the state will confirm that the agency continues to meet all state requirements for Medicare eligibility. CMS will also contact the Fiscal Intermediary to confirm that the agency is located and operating at the physical address indicated on the Medicare application. The hospice agency will then be issued a Provider Number, also referred to as CMS Certification Number (CCN).
In order to bill Medicare, the hospice agency must enroll in EDI and will be issued a Billing Number. We discuss this process separately.
Where can you find more information?
This video from ACHC provides a description of the initial hospice accreditation process
Not everything that looks like a data breach is, in fact, a reportable data breach. Before you report a data disclosure to the US Department of Health and Human Services Office for Civil Rights (OCR), you should confirm that what you are concerned is a reportable data breach is, in fact, a HIPAA breach.
A HIPAA breach is defined as the acquisition, access, use, or disclosure of protected health information (PHI) in a manner not permitted under HIPAA that compromises the security or privacy of the data.
Not every disclosure of PHI is a breach. There are three important exceptions.
Three data disclosures that are not considered a reportable breach:
Unintentional Access:
An employee unintentionally accesses PHI but does not further disclose the PHI in a manner that is not permitted per the HIPAA regulations. For example, a clinician wishes to enter information in the chart for patient “John Smith”. The clinician opens the chart for patient John Smith living on Bay Ridge street instead of patient John Smith living on Reed Street. The clinician closes the chart as soon as the mistake is identified.
Inadvertent Disclosure to Authorized Person:
An individual who is authorized to see the PHI inadvertently shares the PHI with another person in the organization. That second person does not further disclose the information in a manner that is not permitted per HIPAA regulations. For example, a technician sends lab results for the wrong patient to a physician. The physician deletes the results.
Inability to Retain the PHI:
PHI is inadvertently disclosed to someone unauthorized to have access to the information but that person would not be reasonably expected to retain the information. For example, a clinician’s young child is on the phone while the clinician is discussing patient PHI.
Is every disclosure that does not fall into one of these three exception categories considered a reportable breach?
The regulations allow for a four factor analysis to assess the overall level of risk of compromise, to discover the extent of the data breach, and to determine whether or not notification is required. Only after this four factor analysis is completed, the hospice agency determines whether or not a breach occurred and the level of risk.
The following are the four factors:
Factor 1: Nature and Extent of PHI Involved
What information is involved? Can the patients be identified? What personal or helath information is included?
Factor 2: Who Accessed the Data/ to Whom was the Data Disclosed
Was the data disclosed to a person in the organization or in another HIPAA covered organization who is required to follow data privacy rules? In either of these cases, the risk is reduced as both of these types of persons are trained in HIPAA regulations.
Factor 3: Was PHI Actually Acquired or Viewed
Was the PHI actually viewed or acquired? For example, an encrypted device with PHI is stolen but based upon forensic analysis it is determined that no one accessed the PHI. In this case, there was a risk of data breach but analysis determined that PHI was not actually acquired or viewed.
Factor 4: To What Extent have you Mitigated the Risk
What actions have been taken to reduce the risk of PHI access. For example, has the PHI been returned to you? Have you taken steps to track down the device that was not returned by the former employee?
What should I do if a breach has occurred?
If, upon completion of the four factor analysis, it is determined that a breach has occurred, then notification is required.
Affected person must be notified and media and the state may be required to be notified as well.
If fewer than 500 persons are involved, the OCR must be notified at the end of the calendar year. Otherwise, the OCR must be notified within 60 days.
Take appropriate action
Not every disclosure of data is a breach. Investigation must be conducted to determine if the disclosure constitutes a reportable data breach. If the disclosure is a data breach then appropriate actions must be taken to report the breach to all relevant parties within the required time frames. Note that required actions may vary by state.