A Medicare Administrative Contractor (MAC) is a private health care insurer that has been awarded a geographic jurisdiction to process Medicare Part A and Part B medical claims for Fee For Service (FFS) beneficiaries.
CMS relies on these contractors to serve as the primary operational contact between the Medicare FFS program and the health providers enrolled in the program.
MACs are multi-state regional contractors who are responsible for administering Part A and Part B claims.
What types of MACs are there?
There are two types of MACs: Part A/B MACs and DME MACs.
Hospice claims are administered by Part A/B MACs. Part A/B MACs process about 95% of all FFS claims.
There are 12 Part A/B MACs.
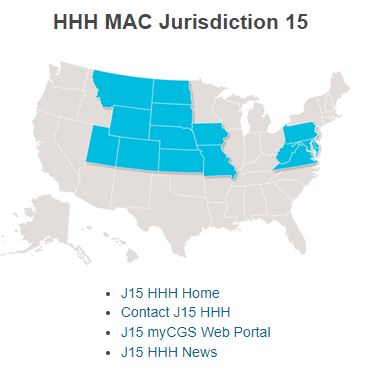
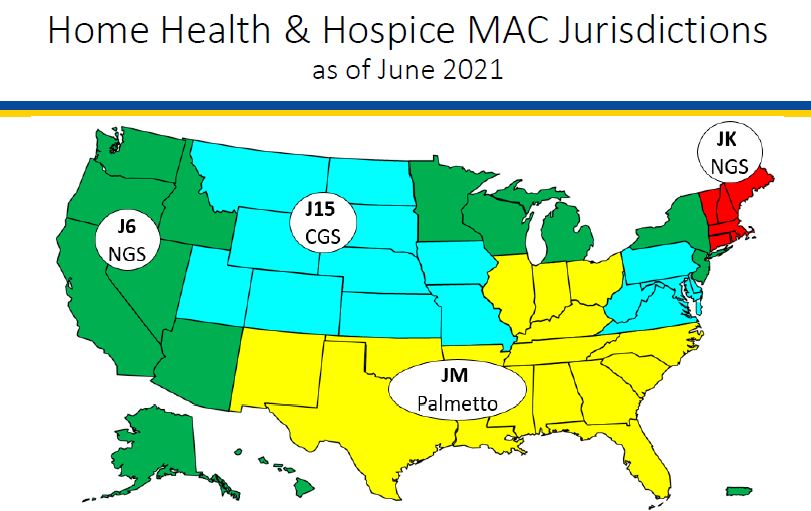
Four of the MACs specialize in processing claims for hospice and home health providers
What geographic areas do each of the hospice and home health MACs cover?
The following map shows the geographic regions that each of the hospice MACs is responsible for administering.
What activities do MACs perform?
MACS perform a number of activities including:
Provider Enrollment
Claims processing, payment, and payment notices
Provider customer service (but not beneficiary customer service)
Audit provider cost reports
Respond to provider inquiries
Audit payments and review medical records
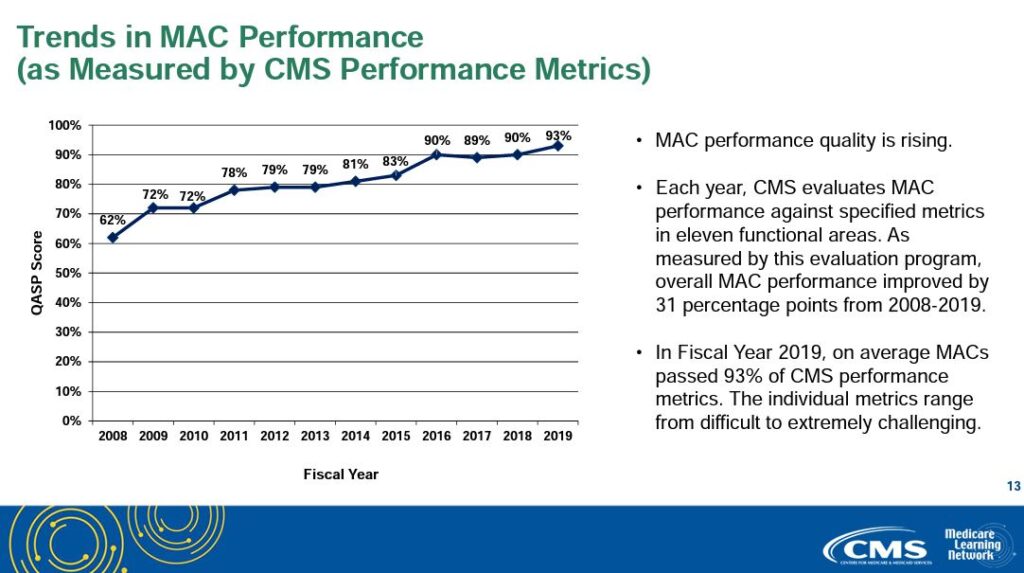
How are MACs measured and how well do they perform?
Each year, CMS evaluates MAC performance against specific metrics in eleven functional areas. MAC performance quality has been consistently improving since CMS began measuring MAC performance. Average MAC performance has increased from 62% to 93% since CMS began measuring MAC performance.
Print ‘n take hospice keys
Seeking to contact your MAC? Here’s their contact information
What is hospice initial accreditation and why is it important?
Hospice initial accreditation is a way to ensure delivery of consistent and high quality services across all accredited hospice agencies. The accreditation program ensures that the hospice agency is fully compliant with Medicare Conditions of Participation. The program also reviews that the hospice is compliant with state and local laws. An on-site survey conducted by the accrediting organization evaluates the quality of the clinical care provided, quality and compliance of patient records, policies and procedures, and performance improvement. Patient and family experiences and quality outcomes are also reviewed. The organization’s financial and long term viability is also studied via review of budgets and other related metrics.
When would a hospice want to complete the accreditation process?
A home hospice must complete the initial Medicare accreditation process before it is able to bill Medicare for services provided to patients. CMS has approved three accrediting organizations (AO) to conduct Medicare surveys and accreditation for hospice agencies: CHAP, ACHC, and JCAHO. These agencies have standardized accreditation and assessment processes although the requirements and actual on-site survey review may vary depending upon state and local regulations.
There are six key elements of the initial accreditation process
File and obtain state home licensure
Register with accreditation organization
Obtain CMS 855A
Develop patient caseload – verify agency is meeting Conditions of Participation
Ensure Conditions of Participation are being met
On-site survey visit
We now discuss each of these elements in greater detail.
Element 1: The process begins with the hospice filing a state home hospice licensure. Each state has its own requirements for approval. So this process and its time lines will differ by state.
Element 2: Register with one of the three accreditation organizations (AO). The AO will require a registration fee. Although the accreditation will be received from CMS, Medicare has granted authorization to AO to conduct the accreditation process on behalf of CMS. The AOs have local branches, allowing them to customize their surveys for state and local regulatory requirements.
Element 3: Confirm 855A is accepted by the Medicare Administrative Contractor (MAC) that is appropriate for the hospice agency’s region: Palmetto GBA, NGS or CGS.
Element 4: Develop patient caseload. Specifically, the hospice must have serviced five patients, with at least three active at the time that the AO conducts the survey. Further, although the hospice is not currently billing Medicare, all patients must be treated as if they are Medicare eligible. All documentation must be completed within the Medicare required time frames and services must be provided by employees, as per Medicare guidelines.
Element 5: Ensure Conditions of Participation are being met. This element involves a number of different items.
The first item is that the hospice agency must verify it is providing all core services using hospice agency employees. Core services include nursing, social work, and counseling including spiritual, bereavement, and dietician. These services must be provided using hospice employees. Contractors may not be used to provide these services. Physician is also a core service but CMS permits the medical director and alternate medical director services to be provided using either hospice agency employees or contracted services.
The second item is to very that the hospice agency is able to provide all non core services using either hospice agency employees or contractors. Non core services include the therapies: physical therapy, occupational therapy, and speech therapy. Additionally, the agency must verify that it is able to provide aide services. It also must be able to demonstrate that it has a bereavement program, even if this service is not yet being used.
The third element is that the hospice agency must verify it can provide all four levels of care including routine, GIP, respite, and continuous care. Not all of these levels of care must be provided through hospice employees; the agency may contract to provide these levels of care.
As a final element, the hospice agency should demonstrate that it can provide DME, pharmaceuticals, drugs and biologicals.
Element 6: On-site survey. Once the hospice confirms that that prior five elements are completed, it will indicate to the AO that it is ready for a Site Visit. The date of the Site Visit will not be announced to the hospice agency but will typically occur within 45 days of when the hospice agency indicates site readiness. The survey will be conducted on-site over three consecutive days. The AO will review patient medical records, accompany staff on patient home visits, and review both clinical and non-clinical hospice agency policies and procedures. The AO will also review the agency for financial viability by reviewing budgets and other related metrics.
What happens after the survey is completed?
After the AO completes the on-site survey, the hospice agency will be notified of the final findings of the survey. There are four possible outcomes.
Agency passed with no deficiencies
Agency passed with minor deficiencies; agency must write an action plan that must be accepted by the accrediting organization
Agency has major deficiencies; deficiencies must be resolved, followed by another three day survey
Agency failed the survey; agency must restart the entire process
What happens after a hospice agency is issued its accreditation letter?
The AO sends a copy of the accreditation letter to the state department of health. Upon receipt, the state will confirm that the agency continues to meet all state requirements for Medicare eligibility. CMS will also contact the Fiscal Intermediary to confirm that the agency is located and operating at the physical address indicated on the Medicare application. The hospice agency will then be issued a Provider Number, also referred to as CMS Certification Number (CCN).
In order to bill Medicare, the hospice agency must enroll in EDI and will be issued a Billing Number. We discuss this process separately.
Where can you find more information?
This video from ACHC provides a description of the initial hospice accreditation process
Cookie Consent
We use cookies to improve your experience on our site. By using our site, you consent to cookies.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga_
ID used to identify users
2 years
_gid
ID used to identify users for 24 hours after last activity
24 hours
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.