Hospice care, since its inception, has been about compassionate care. However, the underlying mechanisms of how it is paid for and how hospice quality is evaluated have undergone a significant transformation. This shift is part of a broader healthcare movement towards value-based care, moving away from simple fee-for-service models. For hospice, this journey can be understood through key eras and events.
1. The Foundation: 1983–2010
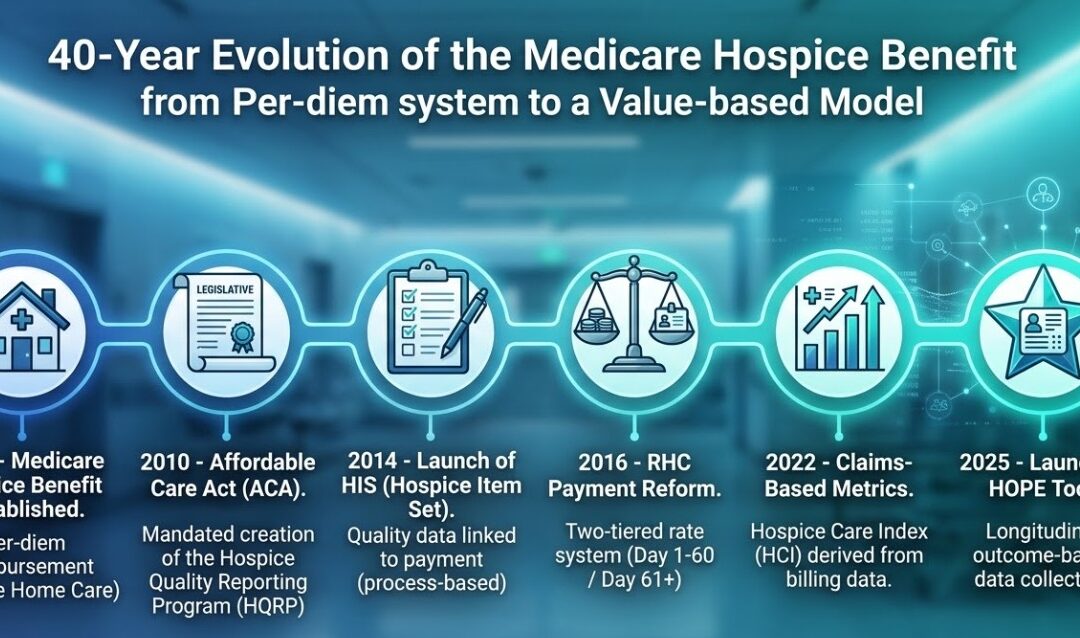
The concept of hospice care solidified with the establishment of the Medicare Hospice Benefit in 1983. This landmark legislation provided a structured way for Medicare beneficiaries to access comprehensive end-of-life care. Originally designed with a primary focus on cancer patients and shorter lengths of stay, it reflected the understanding of terminal care at the time. The reimbursement structure was a per-diem (per day) payment. This model, while straightforward, did not initially distinguish between different levels of care intensity.
The Medicare Hospice Benefit was established in 1983 under the Tax Equity and Fiscal Responsibility Act (TEFRA). For nearly three decades, the payment model was simple: a flat per-diem rate for four levels of care. It was designed for a different era – primarily for cancer patients with short, predictable lengths of stay. During this “Static Era,” CMS had financial data on what they paid, but almost no clinical data on what was actually happening in the home.
2. The Turn Toward Accountability: 2010–2014
As hospice use grew and patient demographics evolved, questions arose about varying practices and quality across providers. This ushered in an era focused on accountability and data collection. The Affordable Care Act (ACA) of 2010 changed the legal landscape. It mandated the creation of the Hospice Quality Reporting Program (HQRP). This marked a fundamental shift, transforming quality reporting from a voluntary endeavor into a mandated requirement for all hospice agencies.
A pivotal moment in this data-driven approach was the 2014 introduction of the Hospice Item Set (HIS). For the first time, agencies were required to submit standardized data on specific quality processes. This also tied hospice quality to payment. Failure to report HIS data resulted in a 2% (now 4%) reduction in the annual payment update.
However, HIS was a “process-based” tool. It measured if a hospice performed an action (like asking about pain), not whether the patient actually improved. Thus, while HIS was a vital step forward, its process-oriented nature was essentially retrospective. It confirmed whether specific admission and discharge procedures were documented, not necessarily if the patient’s well-being improved as a result.
3. Rebalancing the Payment Model: 2016
Parallel to the quality reporting initiatives, CMS implemented structural changes to the hospice payment system itself. In 2016, a significant change was introduced for Routine Home Care (RHC) payments. CMS realized the flat per-diem rate for Routine Home Care (RHC) didn’t match the reality of care delivery. This wasn’t about reducing payments, but about acknowledging the higher intensity of services typically required during the initial 60 days and the final days of a patient’s life.
CMS implemented RHC Payment Reform, creating two separate RHC rates: a higher rate for days 1–60 and a lower rate for days 61+. This was a structural signal that CMS was closely analyzing length-of-stay data and visit intensity. The different per-diem rates were were intended to incentivize a better alignment of payments with actual resource utilization.
Another key milestone was the creation of claims-based metrics. Recognizing the treasure trove of data within existing claims submissions, CMS developed indicators such as those within the Hospice Care Index (HCI). This approach utilized claims data to look for patterns related to care quality, such as the frequency of visits in the last days of life. This represents a clever use of existing data to derive quality insights, moving beyond self-reported assessments.
4. The Era of “Invisible” Metrics: 2022–Present
While agencies were focused on their clinical notes, CMS began using the bills themselves to measure quality. In 2022, they introduced the Hospice Care Index (HCI), a claims-based measure consisting of 10 indicators.
Unlike HIS, which clinicians fill out, the HCI is calculated entirely from existing claims data. This allows Medicare to identify patterns – like “live discharges” or “visits in the last days of life” – without requiring new forms, moving the industry closer to a Value-Based Purchasing mindset.
5. The Failed “Carve-In” and the Path to HOPE: 2021–2025
CMS also engaged in direct testing of value-based models through various pilots and demonstrations. One prominent example was the hospice component of the Value-Based Insurance Design (VBID) Model, often called the “hospice carve-in.” Launched in 2021, Value-Based Insurance Design (VBID) allowed Medicare Advantage plans to manage hospice benefits.
The goals of the VBID hospice carve-in were to assess if integrating hospice within a Medicare Advantage plan could improve care coordination, enhance quality, and reduce spending by preventing unnecessary hospitalizations. This initiative ran until 2024. The insights gained from this experiment, particularly regarding the need for robust quality measures and care coordination, continue to influence the overall direction of hospice payment and quality strategy. The experiment officially ended in December 2024, largely because CMS lacked a standardized, real-time clinical assessment tool to measure outcomes across different plans.
This brings us to the present. The Hospice Outcomes and Patient Evaluation (HOPE) tool, effective October 1, 2025, is the direct answer to this 40-year journey. CMS has finally reached a point where they are no longer satisfied with process checkboxes; they are building the infrastructure to pay for the actual impact of care.
The Path Forward and Why This Matters
The cumulative experiences from these various efforts – the process metrics of HIS, the structural changes in RHC payments, the deployment of claims-based metrics, and the practical learnings from models like VBID – all pointed to a persistent need. The industry required a standardized, patient-centric way to measure actual patient outcomes rather than just processes. This recognized need for more meaningful, outcome-focused data is a direct driver behind the development of the Hospice Outcomes and Patient Evaluation (HOPE) tool, that replaced HIS in late 2025. HOPE aims to capture data longitudinally during a patient’s stay, focusing on symptom impact and goal-setting – providing the rich data environment necessary to genuinely advance value-based care in hospice.
This historical overview illustrates that the shift towards value-based care in hospice is not a recent or sudden development. It has been a steady, deliberate evolution building upon the foundation laid in 1983, constantly striving for a more refined, data-driven system that ultimately ensures high-quality care is both provided and effectively measured. Every regulation, from the ACA to the HOPE tool, has been a stepping stone toward a system that rewards agencies for clinical outcomes rather than just census volume.
Hospice leaders often understand that QAPI is required by CMS, but many do not know how to document the program in a way that proves it is genuinely active and effective. CMS surveyors want to see more than binders, charts, or paperwork. They are looking for documentation that demonstrates continuous, data-driven improvement that is tracked over time. In other words, during survey, they are not just evaluating documents. They are evaluating whether documentation reflects real action.
Why Documentation Matters
In the context of hospice QAPI, documentation is not about filling binders for the sake of compliance. It is about showing that the organization identifies problems, takes measurable action, analyzes results, and adjusts processes accordingly. CMS defines hospice QAPI as a data-based, objective approach to quality management that continuously monitors the outcomes of services, patient safety, and quality of care and requires that providers use this data to design and implement improvement projects when necessary.
To meet this standard, documentation must answer five questions clearly:
What was reviewed
What problem or risk was identified
What action was taken to address it
Whether that action made a difference
What the hospice will do next
If your documentation cannot answer these questions, CMS will not consider the QAPI program compliant, even if the hospice is working hard behind the scenes. The issue is often not that quality work isn’t happening. Rather, the problem is that the work is not being documented clearly enough to show its impact.
Common Documentation Pitfalls
Many hospices get caught in documentation traps that weaken QAPI. They may create binders filled with policies but no records of action, prepare meeting minutes that vaguely state “QAPI discussed” without meaningful content, collect data that is not reviewed or analyzed, or maintain checklists that are completed but not tied to improvement decisions.
These habits create the appearance of a QAPI program without actually demonstrating one. CMS surveyors are trained to recognize documentation that looks like performance but does not show performance.
Start With Defined Indicators
The first step in documenting an effective QAPI program is to begin with defined indicators that are measurable. These indicators form the basis of what the organization monitors and what is documented throughout the year. Examples include pain assessment and management outcomes, timeliness of visits, medication error rates, clinical documentation compliance, grievances or caregiver complaints, and family satisfaction trends. The mistake many hospices make is tracking too many indicators and losing the ability to review and act on them consistently. Monitoring a smaller number or indicators – five to ten well-selected metrics – is more manageable and provides a clearer picture of change over time.
Show How Data Is Reviewed
Once indicators are established, documentation must show how thehospice reviewed data. This is where meeting minutes matter. They should include the date and time of review, the names or roles of participants present, the indicators that were reviewed, and the trends or variances noted. A clear example might read:
QAPI meeting held March 12, 2026. Reviewed late visit data for RN visits Jan–Feb 2026. Findings: 18% of scheduled visits started more than 15 minutes late. Geographic clustering identified in Zone 3. Attending: CEO, DON, QAPI Lead, RN Coordinator.
This simple statement shows activity, data, focus, and context, all elements that demonstrate that QAPI is functioning.
Document Root Cause Analysis, Not Blame
When a pattern or problem is identified, CMS expects hospices to document aroot cause analysis. Root cause analysis is not about blame. Documentation should avoid language that points to individuals as “the problem.” Instead, it should focus on contributors such as workflow bottlenecks, documentation burden, staffing configurations, communication breakdowns, unclear policies, EMR inefficiencies, geographic routing challenges, or training needs.
Tools like “Five Whys” or Fishbone Diagrams can help identify these causes and show depth of analysis. For example, if nurses are repeatedly arriving late, documentation might state:
Primary contributing factor appears to be travel distance; route assignments have not been updated to reflect current census distribution. Documentation burden noted as secondary factor; RNs report medication review template adds charting time. The goal is to show thoughtful analysis, not superficial assumptions.
Record Corrective Actions Taken
After the cause is understood, documentation must show what action was taken.This can be operational, educational, technological, or process-based, but it must be specific and measurable. Documentation should include the intervention chosen, the person responsible for implementing it, and the date it was initiated. For instance:
Action: Adjust RN territory assignments to reduce travel time and reallocate visits in Zone 3. Responsible: Director of Nursing and Operations Manager. Implementation date: March 15, 2026.
This tells the surveyor exactly who acted, what was done, and when. It also provides an anchor point for follow-up measurement.
Prove Results With Re-Measurement
Few steps are more important than re-measurement. This is where many hospices fail. QAPI work is not complete until the hospice checks whether the intervention worked — and documents the outcome. If an intervention does not lead to improvement, documentation should show that the hospice adapted or escalated the intervention rather than abandoning it. CMS does not expect hospices to fix everything on the first try; it expects them to document continuous improvement.
A strong re-measurement entry might read:Re-measured late visit percentage on April 15, 2026. Post-intervention result: Late visits reduced to 9% in Zone 3; hospice-wide reduction to 12%. Action considered effective; monitoring quarterly going forward.
An Example of QAPI Documentation Done Well
When all these elements come together, they tell the story CMS is looking for. Consider a full improvement cycle: On January 20, a hospice identifies a 12% medication documentation error rate during chart audits. In February, EMR templates are revised and staff training is conducted. On March 5, re-measurement shows the error rate has dropped to 3%. This is the type of documentation that proves QAPI is not theoretical. It also shows the hospice is functioning with intention and accountability rather than reacting randomly.
Tools That Support Documentation
The tools used to track this information do not need to be complicated. QAPI meeting minutes, action logs, re-measurement logs, and simple trend charts can meet CMS expectations when used consistently. Many hospices find it helpful to maintain a single “QAPI Action Log” that lists each improvement project from start to finish. CMS offers examples, worksheets, and guidance documents on its website for providers who need structure.
Final Takeaway
Ultimately, documentation should tell a story of how your hospice
Found a risk or opportunity
Tested an intervention
Measured the result
Made further decisions
based on what was learned. When this story can be followed easily and supported with evidence, a hospice has documentation that reflects an active and effective QAPI program. This is the level of clarity CMS expects — not perfection, but proof of progress.
In hospice, most organizations understand why Quality Assessment and Performance Improvement (QAPI) is required. What many do not understand is how to collect data in a way that reveals patterns, risks, and opportunities for improvement.
QAPI data collection does not mean saving every report, printing every dashboard, or drowning in spreadsheets. It means collecting the right information, in the right way, at the right time, so that it provides a story about what is happening inside the organization.
What Data Collection Should Accomplish
A hospice should collect data to answer three essential questions:
What is happening?
Is it getting better, worse, or staying the same?
Does it represent a risk to patients, operations, or regulatory compliance?
If the data that the agency is collecting does not help answer these questions, then either the data points are wrong or the method of collection needs to change.
The Most Common Mistake
Hospices often gather data after a problem has already occurred — almost like autopsy work. That prevents improvement.
Data collection must happen before, during, and after issues appear. Only then can you identify trends and prevent problems instead of reacting to them.
QAPI data can be thought of like a heartbeat monitor: If a patient’s heartbeat is only monitored after the patient has coded, the clinical staff will not have the information that they need to successfully intervene.
What Data Collection Looks Like in Practice
A successful data collection process has three characteristics:
Characteristic
What It Means
Consistent
Collected on a schedule (weekly/monthly/quarterly)
Accessible
Staff can enter information quickly without barriers
Actionable
Someone reviews it and can make decisions from it
Data that is collected but never reviewed is not QAPI; it’s record-keeping.
A Realistic Example
Scenario: A hospice agency is receiving more calls from families stating that nurses are arriving late for scheduled visits.
This is a signal, and signals should trigger structured data collection.
Here is how the hospice agency should approach this in QAPI:
Step 1: Define the Data Point
What should be measured?
Scheduled visit time vs. actual arrival time
This must be collected the same way for every visit being reviewed.
Step 2: Create a Simple, Repeatable Tool
The agency does not need software to begin. A chart, form, or shared spreadsheet is enough:
Patient ID
Date
Scheduled Time
Arrival Time
Late? (Yes/No)
Reason
Reported by
Notes
Step 3: Collect Data Over a Set Timeframe
The agency can decide on the timeframe over which data will be collected: two weeks? one month? one quarter? The timeframe must be long enough to show a trend, but short enough to act quickly.
Step 4: Analyze
After the data is collected, review what happened.
Question
Why It Matters
How often are nurses late?
Shows severity
Are the same nurses repeatedly late?
Training or workload issue
Are late visits tied to geography or routing?
Scheduling issue
Are delays tied to documentation load?
Workflow burden issue
Does lateness correlate with patient complexity?
Staffing model issue
Step 5: Intervene
Example findings → Example actions:
Findings
Action
Late arrivals cluster in one region
Adjust territory planning
Late due to excessive documentation time
Modify EMR workflow or training
Late due to visit volume
Reevaluate caseload standards
Late due to travel time
Redraw service area or change routing
Step 6: Re-Measure
Intervention is not improvement unless data proves it. After the intervention is implemented, the agency must measure again to confirm whether lateness improved. If it did — fantastic. If not — the agency needs to try a new intervention.
This is how QAPI proves effectiveness.
Why This Method Works
This process does three crucial things:
Turns perception (“families say nurses are late”) into measurement
Turns measurement into insight (“where, when, why?”)
Turns insight into action (“fix the problem in the system, not the person”)
When to Start
Intervention and correction of problems identified does not require software systems or large volumes of data. If a hospice is waiting for the “perfect data system,” then the hospice is waiting too long.
Start small.
Start with one data point.
Start even if the first round is messy.
QAPI success begins with a mindset change — not a software purchase.
Takeaway
A hospice agency does not require large volumes of data in order to address issues identified. All that is needed is data that is collected consistently and reviewed with purpose. Data collection is not about volume. It is about visibility.
When data starts showing patterns, it offers the power to prevent problems instead of reacting to them.
A hospice Quality Assessment and Performance Improvement (QAPI) program is the formal system a hospice uses to understand how well it is functioning, where it is at risk, and how it will improve over time. Under 42 CFR § 418.58, CMS requires every hospice to maintain an ongoing, hospice-wide, data-driven program that evaluates the quality and safety of care and takes deliberate action when improvement is needed. In practical terms, a QAPI program is not a set of reports or a compliance binder. It is the structured way a hospice identifies problems, analyzes why they occur, implements changes, and checks whether those changes actually improve care for patients and families.
While the regulation under 42 CFR § 418.58 describes what CMS expects, it does not specify how to build a functioning QAPI program from scratch. The good news is that CMS is not looking for a perfect system. It is looking for a repeatable structure that allows the hospice to identify risk, improve care, and demonstrate learning over time.
The most successful hospice QAPI programs start by putting structure in place before worrying about metrics or dashboards.
What does QAPI mean
At its core, QAPI combines two key components: Quality Assurance (QA) and Performance Improvement (PI). Quality Assurance focuses on setting and maintaining standards of care, while Performance Improvement is about fixing systemic or recurring problems in those care processes. Together, they form a comprehensive, data-driven approach that involves everyone in the organization – clinicians, administrators, and support staff – in practical problem-solving and care enhancement activities. This makes QAPI more than just a regulatory requirement; it is an organized way of doing business that builds quality into every level of hospice operations.
What is the scope of a QAPI program
A hospice QAPI program must be hospice-wide, meaning it must cover all services that affect patient care including clinical services, psychosocial and spiritual care, interdisciplinary group functioning, documentation systems, safety processes, and services provided under contract. The scope of the hospice QAPI program must be defined in writing. The written scope becomes the anchor when questions arise later about whether an issue belongs in QAPI.
The CMS Conditions of Participation require that hospices “collect and analyze patient care and administrative quality data and use that data to identify, prioritize, implement, and evaluate performance improvement projects to improve the quality of services furnished to hospice patients.” This emphasizes the importance of using objective data to show improvement in outcomes, care processes, satisfaction, or other performance indicators.
How does the QAPI program work
A QAPI program begins with data collection. The objective of the data collection is not to accumulate paperwork. Rather, the objective is to reveal patterns, risks, and opportunities for improvement. This can include clinical outcomes, documentation audits, incident reports, grievances, and patient or caregiver feedback. What matters most is that the data allows the hospice to answer key questions:
What is happening?
How often is it happening?
Why is it happening?
What can we do to improve?
QAPI does not require a hospice agency to design a complex data dashboard. It requires identifying reliable data sources that already exist and deciding how they will be used and reviewed.
The agency can start by identifying a small set of core data inputs: patient outcomes, complaints and grievances, adverse events, utilization trends, documentation audits, and patient or family experience data. The goal is not volume; the goal is visibility. When data is reviewed consistently and discussed meaningfully, it becomes usable for improvement.
Identifying concern and monitoring improvements
If an area of concern is identified, the hospice must design and implement an improvement strategy, evaluate the effectiveness of that intervention, and continue monitoring the results over time.
CMS does not require a specific improvement model but it does expect hospice agencies to demonstrate that improvement efforts follow a logical process. The key is choosing an improvement cycle that is easily understood and repeatable and that does not require specialized staff training.
Most hospice agencies succeed by using this straightforward and repeatable sequence:
Identify an issue using data
Analyze why it is happening
Implement a targeted change
Re-measure performance
Monitor whether improvement is sustained
The exact labels are less important than consistency. When the same cycle is used repeatedly, QAPI becomes easier to manage and easier to explain during survey.
What differentiates a strong QAPI program from a weak one is the ability to demonstrate measurable change. Hospice staff and leaders should be able to point to specific improvements that resulted from their QAPI efforts, backed by data over time. This could be a reduction in documentation errors, better pain control outcomes, improved timeliness of visits, or more positive caregiver feedback. These are all examples of real impacts that show the program is not just active, but also effective.
Governance of the QAPI program
CMS places responsibility for QAPI effectiveness on hospice leadership and the governing body. This does not mean that leadership must manage every detail of the QAPI program. What it does mean is that leadership must ensure QAPI operates consistently and has authority.
Leaders are responsible for ensuring that QAPI is integrated into the hospice agency’s policies, procedures, and culture. This includes establishing clear objectives, designating qualified individuals to oversee day-to-day activities, and allocating the resources necessary to support ongoing performance measurement and improvement. The governing body must review QAPI findings regularly and ensure that identified issues are addressed at the organizational level.
Hospice leadership must establish a standing QAPI structure with a regular meeting rhythm and interdisciplinary participation. This can be a formal QAPI committee or a standing agenda item within an existing quality or leadership meeting. What matters is not the name of the meeting, but that QAPI activities are reviewed consistently, decisions are documented, and leadership is aware of priorities and outcomes.
Document how the program operates, not just that it exists
Regulatory compliance is inseparable from solid documentation. CMS surveyors expect to see evidence that a QAPI program is active and effective. Documentation should clearly reflect what was reviewed, what issues were identified, what actions were taken to address those issues, and what the results were. These records should show the agency’s ability to track performance and demonstrate improvement over time.
A QAPI program that exists only in manuals or binders but lacks real, documented improvement activities will be seen as ineffective during survey. Strong documentation tells the story of improvement over time. It shows that QAPI is active rather than simply theoretical. This becomes critical during survey, when the hospice must demonstrate not only intent, but execution.
Why QAPI Matters Beyond Compliance
While QAPI is a regulatory requirement, its impact extends far beyond mere compliance. When implemented thoughtfully, a QAPI program becomes a strategic advantage for a hospice agency. It enhances care quality, strengthens patient and family satisfaction, and supports organizational resilience in a rapidly evolving healthcare environment.
A hospice that can continuously monitor performance, learn from data, and act proactively is better positioned to deliver high-value, person-centered care every day. In an era where quality reporting and public transparency are increasing – including through programs like the Hospice Quality Reporting Program (HQRP), which publicly reports data on hospice performance measures – hospices that embrace continuous improvement are likely to stand out in quality metrics and community reputation.
The initial comprehensive assessment is more than a routine procedure; it is the cornerstone of every hospice care plan. For providers and administrators, understanding the full scope of this assessment is critical, as it serves as the primary data point for compliance, effective care delivery, and risk mitigation.
According to Medicare hospice requirements, a comprehensive assessment must be completed by a Registered Nurse within 48 hours of a patient’s election of services. This is not merely a box to be checked; it is a vital step for confirming eligibility, guiding the care plan, and ensuring that all aspects of the patient’s condition and needs are thoroughly documented for the entire interdisciplinary team.
Key Components of a Compliant Assessment
A rigorous, multifaceted assessment is essential for capturing the data needed to build a robust and defensible care plan. Key areas of focus include:
Terminal Condition: A clear assessment of the patient’s terminal illness and its progression is required to establish clinical eligibility.
Risk Factors: Identifying medical and psychosocial risks is crucial for proactive care planning and avoiding adverse outcomes.
Functional Status: Documenting the patient’s mobility, self-care capacity, and overall functional status provides the baseline for tailored interventions.
Imminence of Death: An honest and well-documented assessment of the patient’s prognosis helps the clinical team prioritize immediate and ongoing care needs.
Symptom Severity: A thorough evaluation of symptoms such as pain, nausea, and fatigue is necessary to implement effective symptom management protocols.
The Drug Profile and Documentation
A critical element of the initial assessment is a meticulous review of the patient’s entire drug profile, including prescriptions, over-the-counter medications, and alternative treatments. This step ensures medication effectiveness, identifies potential side effects or harmful interactions, and prevents duplicate drug therapy. Proper documentation here is essential for compliance and maintaining an accurate care record.
Gathering Comprehensive Data: Beyond the Chart
While the RN leads the assessment, the process involves gathering critical input from all relevant stakeholders. This collaborative approach ensures the care plan is based on a complete clinical picture.
Patient-Centered Data: The RN must engage the patient to understand their preferences, fears, and goals, respecting their autonomy in all care decisions.
Caregiver & Family Input: Caregivers provide invaluable firsthand knowledge of a patient’s daily condition and challenges. Engaging them in the assessment process yields crucial insights that may not be available elsewhere.
The Bereavement Assessment
The initial assessment also requires a formal evaluation of the family’s bereavement needs. This step, often led by the social worker or chaplain, gathers information on social, cultural, and spiritual factors that will impact how the family copes with loss. This is a non-negotiable part of the assessment that ensures the hospice team can provide comprehensive support.
Time Required for the Initial Comprehensive Assessment
The initial comprehensive assessment typically takes 1 to 2 hours to complete. The time required can vary depending on the patient’s condition and the complexity of their medical and psychosocial needs. The nurse will need time to gather detailed information, assess the patient’s symptoms, and discuss treatment options with the family. This assessment is an essential process, ensuring that all aspects of the patient’s care are considered, and an appropriate hospice care plan is developed. Additionally, thorough documentation is needed to meet Medicare requirements, ensuring that the care plan reflects the patient’s needs accurately.
A Foundation for Quality and Compliance
The initial comprehensive assessment is not a one-time event; it is the first link in a chain of continuous care. The data collected forms the basis for the entire interdisciplinary team’s plan and is revisited through ongoing assessments.
For administrators and clinicians, the two hours dedicated to this process are an investment in the organization’s integrity. A meticulous assessment ensures compliance with Medicare guidelines, improves the quality of patient care, and ultimately supports the hospice’s ability to operate with excellence.
Additional Resources
CMS eCFR on Hospice Assessments: This is the direct source for the federal regulations governing hospice care. It outlines the specific requirements for the initial and comprehensive assessments, including deadlines and content standards. It’s an essential reference for compliance officers and administrators. (42 CFR 418.54 — Condition of participation: Initial and comprehensive assessment of the patient. – eCFR)
CMS Hospice Comprehensive Assessment Quality Measure: This fact sheet from the Centers for Medicare & Medicaid Services (CMS) explains the “all or none” composite measure used to evaluate a hospice’s performance on the comprehensive assessment. It’s a critical document for understanding quality reporting and performance improvement programs. (CMS Hospice Comprehensive Assessment Quality Measure)
Accreditation Commission for Health Care (ACHC): This article provides an overview of how to complete a compliant comprehensive assessment, drawing on both Medicare Conditions of Participation (CoPs) and ACHC standards. It offers practical guidance for RNs and clinical leaders. (Completing a Comprehensive Assessment for a Hospice Patient)
Hospice Eligibility Guidelines from VITAS: This resource is particularly useful for clinical staff, as it provides detailed, disease-specific guidelines for determining hospice eligibility. It’s a practical tool for nurses and medical directors during the initial assessment. (Hospice Eligibility Guidelines for HCPs – VITAS Healthcare)
Hospice agencies are under increasing scrutiny by government auditors. A particularly concerning and financially devastating aspect of government audits is the use of statistical extrapolation. Understanding the extrapolation process is essential for providers to safeguard the financial healthof their agencies and ensure compliance with all regulations.
What is Government Extrapolation in Hospice Audits?
Extrapolation is a statistical methodology used by auditors, particularly the Office of Inspector General (OIG). Extrapolation can significantly amplify the financial implications of audit findings. The process of extrapolation is governed by the Medicare Program Integrity Manual, Chapter 8. This chapter of the manual outlines the specific statistical methods and requirements for conducting extrapolation studies.
What is Extrapolation?
Extrapolation is a sampling technique used to project audit findings from a small sample of claims to an entire population of claims. Instead of reviewing every single claim that a hospice has submitted for payment, auditors select a statistically valid sample for review. They then use the error rate found in the sample to estimate overpayments across all similar claims in the population. This allows auditors to perform a detailed review of only a small sample of claims while estimating the total amount of improper claims across a large population.
Auditing every single claim in the population is impractical due to time and resource constraints. By examining a representative sample, auditors can make statistically valid projections about a much larger group of claims without having to review each one individually.
How Does the Extrapolation Process Work?
The extrapolation process typically follows the following key phases:
Universe Definition:
Auditors define the “universe” or population of claims to be examined. This may be all Medicare hospice claims submitted by your agency within a specific period (e.g., all claims billed between January 1, 2024, and December 31, 2024) or a subset of claims (e.g., all General Inpatient Care claims).
Sample Selection:
Using statistical sampling software, auditors select a statistically valid random sample from the universe. The term “statistically valid” is significant because it ensures that the sample accurately represents the entire population. This allows for reliable projections from the sample to the larger group. The industry standard software used to support sample creation is called RAT STATS (created by the OIG for the U.S. Department of Health and Human Services). Typically, samples consist of 100 claims, though this can vary.
Medical Review:
Each claim in the sample is rigorously reviewed by independent medical contractors who determine whether the services provided met Medicare requirements for hospice eligibility and documentation. The auditors review the documentation for compliance with Medicare regulations, including patient eligibility, physician certifications, medical necessity for services, and appropriate billing for levels of care. Any claim found to be out of compliance is identified as an “error,” and the precise dollar amount of the overpayment for that specific claim is calculated.
Calculation of Error Rate:
A monetary error rate is determined for the sample. This is calculated by dividing the total dollar amount of improper payments found in the sample by the total dollar amount of payments for all claims in the sample.
Extrapolating to the Universe/Statistical Projection:
The calculated monetary error rate from the sample is applied to the entire “universe” of claims. This projects the estimated total overpayment across all claims in the defined audit scope. The estimated total overpayment is calculated as the monetary error rate of the sample multiplied by the total dollar paid for the audit universe.
How Does Extrapolation Impact a Hospice Agency?
Extrapolation can have a significant financial impact on hospice agencies. Even a small number of denied claims or identified overpayments in a sample can result in a large demand for repayment. This can pose a severe financial challenge. Further, responding to an extrapolated audit can pose a significant administrative burden on hospice agencies, requiring considerable time and resources from administrative and compliance teams.
Additionally, OIG audit findings are often publicly released. This raises concerns about agency reputational risk and may jeopardize relationships with referral sources and the community. An adverse extrapolated audit outcome can also lead to increased scrutiny in future audits and potentially trigger further investigative actions.
Mitigating Extrapolation Risk
Given these potential significant negative impacts of extrapolation, hospice agencies should consider proactive actions that could help mitigate the likelihood of negative audit findings. The most effective actions include:
Robust Compliance Program: Agencies should implement and strictly adhere to a comprehensive compliance program. This includes continuous staff education on Medicare regulations, thorough patient eligibility assessments, diligent documentation of physician certifications, and accurate coding for all levels of care.
Internal Auditing: Conduct regular, proactive internal audits of claims and medical records. Focus on high-risk areas identified by Medicare (e.g., General Inpatient Care (GIP) stays, long lengths of stay, live discharges). Identifying and correcting deficiencies internally before an external audit is crucial.
Looking Ahead
Government extrapolation in hospice audits represents a significant financial risk for hospice agencies. Understanding the statistical methodologies, maintaining excellent documentation practices, and implementing robust compliance programs are essential for surviving in this challenging regulatory environment.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga_
ID used to identify users
2 years
_gid
ID used to identify users for 24 hours after last activity
24 hours
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.