by editor | Aug 3, 2024 | Compliance and Regulatory - Directors, Human Resources, Regulatory Compliance
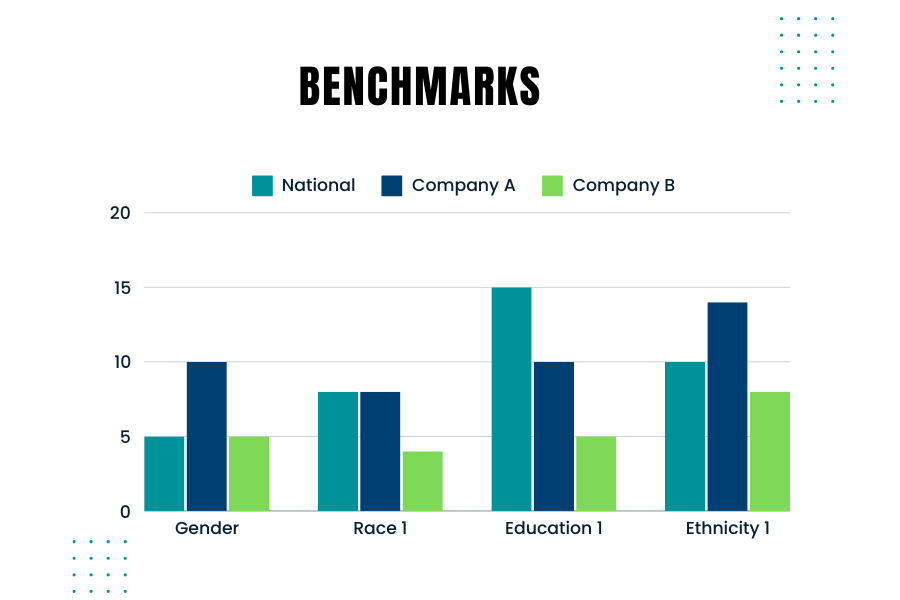
Creating and using benchmarks to compare your company’s hiring demographics against those used by government agencies like the EEOC (Equal Employment Opportunity Commission) is crucial. Benchmarking helps ensure that your company’s hiring practices are fair and compliant with federal regulations. Here’s are some considerations to keep in mind when you consider the right benchmarks
Why Benchmarking Matters
Government agencies monitor and require companies to report on the demographic composition of their workforce, especially larger companies. For instance, the EEOC uses benchmarks to compare a company’s demographics against broader population data from sources like the U.S. Census and the American Community Survey. Knowing how your company’s demographics stack up against these benchmarks is essential for several reasons:
- Compliance: Ensuring your hiring practices comply with laws such as the Civil Rights Act and the Age Discrimination in Employment Act.
- Diversity Goals: Meeting your company’s diversity and inclusion goals.
- Fair Hiring Practices: Ensuring fair and unbiased hiring practices.
Best Practices for Benchmarking
- Collect Internal Data: Gather detailed demographic data of your current workforce and applicants.
- Ensure you track data on race, gender, age, and other relevant demographics.
- Choose the Right External Data: Depending on your hiring scope, use national, regional, or local data. For example, if you recruit nationwide, use national benchmarks. For local hires, consider regional data.
- Occupation and Industry-Specific Data: Align your benchmarks with the specific occupations and industries relevant to your company. Different industries and roles may have distinct demographic compositions.
- Adjust for Educational Requirements: Consider the educational requirements for the roles you are hiring. This will help you compare your applicant pool against the qualified population.
- Use Census Data: The U.S. Census Bureau provides comprehensive data that can be segmented by occupation, geography, and other factors. This data is a good starting point for creating your benchmarks.
Ensuring Fair Selection
To avoid over- or under-selecting any protected group, follow these steps:
- Regularly Update Benchmarks: Demographic data changes over time. Ensure your benchmarks are based on the most recent data.
- Monitor Hiring Practices: Continuously monitor your hiring practices and outcomes against your benchmarks.
- Training and Awareness: Educate hiring managers on the importance of diversity and compliance with hiring practices.
External Data Sources
Looking at external data sources is important because it provides a broader context for your internal data. It helps you understand the labor market and demographic trends in your industry and location. External benchmarks serve as a snapshot of the current workforce composition, which can change over time.
Creating effective benchmarks involves a blend of using accurate external data and understanding your company’s unique needs. By comparing your company’s demographics against reliable benchmarks, you can ensure fair and compliant hiring practices. Regularly updating these benchmarks and educating your hiring team on best practices will help maintain a diverse and inclusive workforce.
Where Can You Find Additional Information?
- Of Significance: Don’t Miss the Mark! Podcast on what to keep in mind when creating benchmarks
- Harvard Business Review: Smart benchmarking starts with knowing whom to compare yourself to

by editor | Feb 14, 2024 | Compliance and Regulatory - Directors, Regulatory Compliance
The hospice Special Focus Program (SFP) is conducted by the Center for Medicare and Medicaid Services (CMS). The objective of this program is to identify poor performing hospice agencies, based upon quality indicators, that place hospice beneficiaries at risk. These hospice agencies will then be subject to additional scrutiny and oversight to ensure that they meet Medicare requirements. The SFP is designed to either bring these programs into compliance or force them out of the Medicare program by terminating their Medicare status.
What is the origin of the Special Focus Program?
The hospice Special Focus Program was mandated in the Consolidated Appropriations Act of 2021. That is also when it was clarified that hospices would be surveyed every three years. All hospices now have had a survey since 2021. Some of that data is being used for the hospice Special Focus Program, which is designed to identify the worst performing hospices and either bring them into compliance or force them out of the program by terminating their Medicare status.
How is a hospice agency selected for inclusion in the Special Focus Program?
CMS uses an algorithm to identify the poor performing hospice agencies to include in the SFP. The algorithm combines data from a few data sources to score each of the hospice agencies. The score is based on data from: condition-level deficiencies in standard surveys, substantiated complaints, Hospice Care Index (HCI), and the CAHPS survey. The algorithm does not stratify hospice agency based upon size or location; all hospice agencies are held to the same standard regardless of their size or location. The bottom 10% ranked hospice agencies (which are the hospice agencies with the highest algorithm score) are selected to be included in to the SFP.
What is the impact of a hospice agency being included in the SFP?
Hospice agencies that are included in the SFP will be publicly reported on the SFP website. SFP is a framework for increased oversight. The hospice agencies that are included in the SFP program will be surveyed more frequently — at least every six months. CMS will determine what actions must be taken based upon the survey results.
How will a hospice agency exit the SFP?
A hospice will complete the SFP if in an 18-month time frame the hospice agency has no Quality of Care condition level deficiencies or immediate jeopardies for any two six month SFP surveys and has no pending complaints or have returned to substantial compliance with all requirements. The hospice will receive a letter from CMS that will indicate official completion of the program. If a hospice is unable to meet the completion criteria – due to inability to successfully pass surveys or continued complaints while on the SFP – it will be placed on the Medicare termination track.
Even as hospices work to improve their levels of quality and compliance, there will always be hospice agencies that fall in the lowest 10% of performance relative to their peers. Only by continually monitoring their quality performance and comparing these quality scores to peer performance can a hospice agency stay out of the lower 10% and off of the SFP list.
Where can you find out more?
Hospice Special Focus Program – CMS
by editor | Mar 22, 2023 | Compliance and Regulatory - Directors, Metrics and KPIs, Rules and Regulations - Nurses, Rules and Regulations - Office Team
Patient length of stay is monitored to detect instances of inappropriate use of the hospice benefit or other deficiencies in the services delivered by the hospice provider. Length of stay is monitored for both very short length of stay as well as for length of stay that is longer than the norm.
What may unusual length of stay tell a hospice provider?
When patients are discharged alive with a short length of stay it may signal that the patient did not understand the hospice benefit when the patient was admitted to hospice. Or, patients may discharge live from hospice after just a few days because they were not satisfied with the services delivered by the hospice provider. Patients with length of stay longer than 180 days could be indicative of a patient who is no longer hospice eligible. Patients who are no longer eligible for service should be discharged from hospice and any payments that were received from Medicare while the patient was no longer eligible for services should be returned to Medicare. Failure to discharge the patient or failure to return the funds are examples of fraud and abuse.
How is length of stay calculated?
Length of stay is calculated based on the number of days that a patient receives hospice care. Specifically, for a patient who is discharged from hospice (whether or not the patient is discharged alive), the patient length of stay is calculated as follows:
Patient length of stay = [patient discharge date]-[patient admission date]+1
Which patients are included in length of stay calculation?
The length of stay calculation assumes that only discharged patients are considered in the calculation – since the formula expressly refers to the patient discharge date. When only discharged patients are considered (whether live discharges or discharges due to death), the hospice provider only has a backward-looking view on performance relating to length of stay. For example, if a hospice provider has been providing service to a patient for 12 months and the patient is still on service, the patient will not be included in the traditional average length of stay metric – since the patient has not yet been discharged. On the other hand, once the patient is discharged the patient’s length of stay will be at least 365 days since the patient – while still currently active – has already been on service for 365 days. If active patients are considered in a length of stay calculation, it gives a hospice provider a metric that can be used to highlight patients whose clinical charts and documentation of care may benefit from additional review.
What length of stay metrics should be calculated?
In addition to computing average and median length of stay based on discharged patients only, average and median length of stay can be computed for active patients. Patient length of stay for an active patient is calculated as follows:
Active patient length of stay = [end of evaluation period date]-[patient admission date]+1
For example, suppose the current date March 15, 2023 and a hospice wishes to calculate the active patient length of stay as of the end of 4Q 2022 for a patient who was admitted on December 1, 2022. The calculation is as follows:
- End of evaluation period date: 12/31/22
- Patient admission date: 12/1/22
- Active patient length of stay = (12/31/22) – (12/1/22) + 1 = 31 days
The active patient length of stay as of the end of 4Q 2022 is 31 days.
If the hospice wishes to calculate the active patient length of stay as of current date, the calculation is as follows:
- End of evaluation period date: 3/15/23
- Patient admission date: 12/1/22
- Active patient length of stay = (3/15/23) – (12/1/22) + 1 = 105 days
Average and median length of stay would be computed as usual. If any concerning value — such as long length of stay – is identified based upon the active patient length of stay, a hospice provider can immediately investigate and determine if any remediation action is required, rather than waiting until patients are discharged. Delay can lead to additional fines or further action from Medicare.
by editor | Mar 22, 2023 | Compliance and Regulatory - Directors, Metrics and KPIs, Rules and Regulations - Nurses, Rules and Regulations - Office Team
Patients are eligible for hospice if they have a terminal diagnosis and a prognosis of six or fewer months to live if their disease runs its natural course. A patient who lives longer than six months can still get hospice care if the medical director or other hospice physician recertifies that the patient is still terminally ill.
What is hospice patient length of stay?
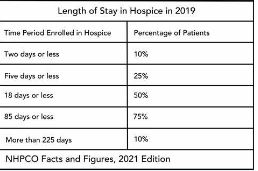
Hospice length of stay is an important metric that is monitored by both CMS and by hospice providers. Hospice length of stay measures the count of days that a patient receives hospice services, from the day that the patient is admitted into hospice until the day the patient is discharged (either alive or deceased). In 2018, 25% of Medicare beneficiaries received hospice care for seven days or less and 54% of Medicare beneficiaries received hospice care for 30 days or less.
Why should a hospice monitor patient length of stay?
Monitoring patient length of stay can aid in detecting cases of possible fraud or abuse – instances where ineligible patients continue to receive the hospice benefit. This metric also helps monitor whether the hospice benefit is being adequately utilized. Although patients are eligible for hospice when they have six months or less to live, most patients receive less than 30 days of hospice care.
Agency patient length of stay is also trended over time and is also compared against the value for patients in the same region, state, or nationwide. The metric may also be analyzed for patients in subpopulations – for example patients with the same disease, race, or ethnicity.
How is patient length of stay calculated?
Patient length of stay is calculated using all patients discharged by the hospice provider during the reporting period. For example, if the hospice would like to compute the length of stay for patients during the 4Q 2022, all patients who were discharged during 1Q 2023 would be included in the calculation. For each patient, the number of days from the date of patient admission until the date of patient discharge is counted; this represents the patient length of stay.
Patient length of stay = [patient discharge date]-[patient admission date]+1
What are common measures of length of stay?
Two common patient hospice length of stay measures are Average Length of Stay (ALOS) and Median Length of Stay (MLOS).
Average length of stay
Average length of stay is the arithmetic mean of the data collected. Specifically, if d is patient length of stay and N is the total number of patients then average length of stay (ALOS) is calculated as follows:
ALOS = ( d1 + d2 + d3 + …. + dn ) /N
Where di = patient length of stay for patient i
Median length of stay
Median length of stay is the middle number in the sequence of numbers. Specifically, compute the length of stay for all N patients. Then, order these N numbers in ascending order. The middle number is the median. If the number of patients is even then there is no middle number. Instead, the median is calculated by taking the average of the two numbers in the middle.
Comparing average and median length of stay
The average is sensitive to outliers in the data. That is, if there are a few patients with a very high length of stay while all other patients have a significantly lower length of stay, the average will be biased by these outliers and will give a misleading assessment of overall patient length of stay. Below, we give an example to provide greater intuition into the impact of outliers on average length of stay and the difference between mean and median length of stay.
Suppose a hospice agency discharged 35 patients during 4Q 2022. The patients’ lengths of stay are as follows:

We compute the average length of stay by summing each of the 35 patient’s length of stay (in the “Length of Stay” column) and dividing that total by 35 (the total count of patients).
Average length of stay (ALOS) = 38.5
We compute the median length of stay by sorting the patient’s length of stay in ascending order and identifying the central number. Since there is an odd number of patients, there will be a single central value. In this case, the central value is 20.
Median length of stay (MLOS) = 20
Average length of stay is almost double the median length of stay. What is leading to these significant differences between ALOS and MLOS? Observe the outliers in the data. There are two patients with length of stay that exceeds 200 days. There are two additional patients with length of stay exceeding 100 days. Since ALOS is sensitive to outliers, ALOS is being pulled to a higher value due to the presence of these outliers.
To provide additional insight, we have plotted a histogram of the length of stay values. A histogram shows the count of observations in the data that fall in each of the specified ranges.

The table on the left shows the count (frequency) of observations of patient length of stay in the data for each of the ranges: 0-10 days, 10-20 days, 20-30 days, 30-40 days, and greater than 40 days. There are 11 patients with length of stay between 0-10 days, 7 patients with length of stay between 10-20 days, 6 patients with length of stay between 20-30 days, 6 patients with length of stay between 30-40 days, and 4 patients with length of stay that exceeds 40 days.
Think about this histogram and now consider the MLOS and ALOS. Median length of stay is 20 days – it falls well in the middle of the data. Average length of stay, however, equals 38.5. It falls, essentially, in the final bar of this histogram and well beyond where the majority of the data lies. The provides a visual demonstration of the impact of outliers on ALOS.
Providers should monitor both ALOS and MLOS. Significant differences between these numbers would indicate the presence of outliers and should be investigated.
Print ‘n take hospice keys
- Understanding the difference between the average (mean) and the median
Where can you find out more?

by editor | Jan 29, 2023 | Compliance and Regulatory - Directors, Metrics and KPIs
Why is data valuable?
Like all other business decisions, a hospice marketing plan must be data driven. More progressive hospice agencies have increasingly begun to understand the value of many types of data in supporting business decisions. This includes internal data such as patient EMR data, financial data including general ledger revenue and expense data (at various levels of aggregation), and quality data. It also includes external data such as publicly available claims data, cost report data, and referral data.
This article published in June 2021 discusses how hospice agencies are using data analysis as a tool to gain an edge over competitors when engaging with potential referral sources. The discussion focuses on use of data analysis to identify which physicians represent referral sources that are more likely to produce (higher quality) referrals. This 2016 NHPCO article discusses the use of hospice metrics as a marketing tool. For example, a hospice agency can share statistics on reduction in hospital admissions for its patients in hospice compared to hospital admissions prior to hospice admission. Other metrics on cost of care or patient satisfaction are of interest, depending upon the referral source.
What data is valuable for designing a marketing strategy?
A hospice should gather data so that it can develop a complete picture of the customers that it serves. It should analyze its patients – including referral sources and patient attributes such as patient diagnosis, length of stay, and patient demographics. Referral sources can be analyzed at different levels of aggregations such as geographic location, facility type, physician type, and physician name. Analysis of hospice patients should be compared to analysis of data for the entire market (in the relevant geographic region). This can help a hospice agency identify where it may have strengths or weaknesses and contribute to its marketing strategy.
Analyze the data: gain input from multiple sources
When analyzing the output of the data analysis, the hospice agency should solicit input from multiple sources in the organization. Combining different perspectives on the data such as input from the executive, marketing, and clinical teams will provide a more holistic view and a more accurate assessment of the current marketing performance and how the go-forward marketing strategy should be designed.
How can the data be analyzed?
The simplest method for analyzing the data is to use Microsoft Excel. Excel is widely used in most organizations, so gaining access to this software should not be difficult. With relatively simple commands, one can analyze data and create charts to visualize the results of data analysis. Another benefit of using Excel for data analysis is that a lot of educational material is available on the Web to answer any questions that you may have about using Excel – in case there are data analysis functions that you want to learn more about.
What other information may be relevant to developing a strategy?
Patient data and claim data are historical data that are important inputs to a developing a marketing strategy. A hospice agency should also analyze forward-looking data as well as more general information such as:
- What are hospice market trends in the geographic region?
- How competitive is the marketplace and are there expectations for change in competition in the near term?
- How well is the role of hospice understood by communities in the geographic region?
- Is the use of hospice accepted by communities in the geographic region?
- Is hospice understood by the medical community in the geographic region?
- What are the demographics of your geographic region and are they expected to change in the near term?
Combining analysis of historical and forward-looking data and soliciting input from team members with different perspectives such as operational, clinical, and marketing will help a hospice agency develop an effective marketing plan.
Where can you find out more?
Using hospice metrics for marketing
by editor | Jan 29, 2023 | Compliance and Regulatory - Directors, Hospice 101 - Aides, Hospice 101 - Chaplain, Hospice 101 - Nurses, Hospice 101 - Office Team, Hospice 101 - Social Workers, QAPI, Regulatory Compliance
What is the governing body?
In accordance with the Conditions of Participation, a Medicare certified hospice agency must have a governing body. The governing body has ultimate responsibility for the hospice agency, including legal and financial authority. Medicare Conditions of Participation require that the governing body is informed of the ongoing activities at the hospice agency, including patient care delivery issues and all QAPI activities. The governing body must also appoint a qualified hospice administrator – a hospice employee with the necessary education and experience – who is responsible for hospice daily operations.
The governing body must meet at least quarterly and must maintain written minutes of its meetings.
There are two Conditions of Participation – 418.100 and 418.58 – that relate to the hospice governing body.
Condition of Participation 418.100
This Condition of Participation defines a standard that the governing body is responsible for management of the hospice agency, including its fiscal operations, provision of services, and continuous quality assessment and performance improvement (QAPI) efforts. The governing body also assumes full legal authority of all hospice operations. It further specifies that the governing body should appoint an administrator that reports to the governing body and who is responsible for hospice agency daily operations. The hospice administrator must be a hospice employee and must have necessary training, education, and experience. CMS does not specify the process by which an administrator should be selected by the governing body. If a hospice agency has multiple locations, the governing body is responsible for administration, supervision, and services for all locations as well as for any arranged services.
Condition of Participation 418.58
This Condition of Participation discusses requirements of a hospice agency’s QAPI program. The governing body must ensure that the hospice agency maintains and implements an ongoing quality improvement and patient safety program. Program performance must be monitored on a regular basis. Further, the governing body must ensure that one or more individuals are selected to lead the organization’s QAPI efforts.
The hospice agency’s organization documents must specify that the hospice governing body is responsible for the QAPI program. Additionally, the governing body specifies the frequency of data collection and level of detail of data collected by the QAPI program.
Are there any state regulations?
State hospice licensure regulations may impose additional requirements on the hospice governing body. They may also have specific requirements on the administrator that is selected by the governing body. A hospice is required to meet the most stringent requirements (whether state or federal).
Surveyors will check that all conditions are met. A hospice agency should maintain evidence of the governing body’s role and activities. Governing body authorizations and activities should be documented in governing body meeting minutes, company organization documents, and company policies and procedures.
Where can you find out more?
CMS Conditions of Participation – Governing Body
