

The PEPPER report target areas focus on statistics that will identify potential for improper Medicare billing. Comparison to national, jurisdictional, and state percentiles can highlight a hospice agency’s potential need for change to its practices to guard against improper billing. Hospice agencies can leverage the information on these reports to prioritize internal audit and efforts to ensure accurate billing.
Why did CMS focus on the target areas in the PEPPER report?
- Concern: Are patients eligible and is the agency providing good quality of care?
- Target Areas: Live discharges – no longer terminally ill or patient revocation
- Discussion: A hospice may discharge a patient alive because the patient is no longer eligible, the patient revoked, the patient moved out of the service area, or for cause. The first two reasons are concerning. These reasons for live discharge may indicate that the hospice is admitting patients who are not hospice eligible. If the patient revoked it may indicate that the quality of care is lacking.
- Concern: Is a hospice agency trying to take advantage of the high routine home care rate?
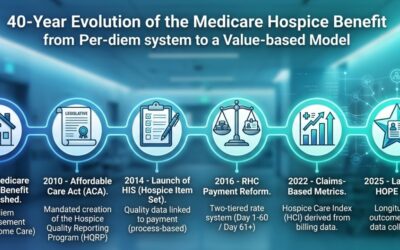
- Target Area: Live discharge with length of stay between 61-179 days
- Discussion: CMS pays a higher rate for the first 60 days of routine home care; the rate of payment is lower for days 61+. High incidence of live discharge in days 61+ may indicate the hospice agency is driven by financial concerns and wants to discharge patients once the rate drops.
- Concern: Is the hospice agency admitting ineligible patients?
- Target Area: Long length of stay
- Discussion: The hospice may be admitting ineligible patients and therefore have an unusually long length of stay as compared to its peers
- Concern: Is the hospice agency targeting patients in more profitable care settings?
- Target Area: Services provided in assisted living facilities
- Discussion: An OIG study published in January 2015 found that Medicare payments for hospice care to patients in assisted living facilities increased significantly. While the diagnoses of patients in this setting typically involved less complex care, these patients remained on hospice longer and hospices received higher payments than for patients in other settings. There is therefore a need to monitor whether hospices are targeting patients in more profitable care settings including assisted living facilities, skilled nursing facilities, and nursing facilities.
- Concern: Is a hospice agency accurately reporting all diagnoses on the claim?
- Target Area: Claims with a single diagnosis code:
- Discussion: A hospice should report on the hospice claim the principle diagnosis and all diagnoses related to the terminal illness and related conditions. A hospice agency that has an unusually high number of claims with a single diagnosis may indicate that the hospice is not reporting all related diagnoses.
- Concern: Is the hospice agency meeting Medicare CoP and able to offer all four levels of care?
- Target Area: No general inpatient or continuous home care
- Discussion: Medicare Conditions of Participation require hospices to demonstrate they can provide all four levels of care: routine home care, general inpatient care, inpatient respite care, and continuous home care to be a Medicare certified hospice provider. A report published by CMS in 2014, included an analysis of 2012 hospice claims:
- 3% of beneficiaries did not have any general inpatient care in 2012
- 1% of hospice agencies did not provide any general inpatient care to any of their patients
- 4% of all hospice days billed in 2012 were billed as continuous home care
- 7% of hospice agencies billed at least one day of continuous home care but the share of continuous home care days billed varied across hospice agencies that billed any continuous home care days
- Almost 90% of hospice agencies that provided continuous home care had less than 1% of their days billed as continuous home care
- Four hospices billed more than 10% of their days as continuous home care.
This target area aims to monitor that hospice agencies are meeting the hospice Conditions of Participation and are able to provide all four levels of care.
- Concern: Is general inpatient care being used appropriately and are patient symptoms being managed well?
- Target Area: Long general inpatient stays
- Discussion: General inpatient stays are intended to be short term, to treat acute symptoms. If a patient has extended general inpatient stay there this level of care is not being used appropriately or that symptoms are not being properly managed.
- Concern: Is Medicare making prescription drug Part D payments when these should be paid by the hospice agency?
- Target Area: Medicare Part D payments for hospice beneficiaries
- Discussion: Hospice agencies are paid a per diem rate for each day that a patient is in hospice care, irrespective of the services that the hospice agency provides to the patient. Drugs that the hospice agency provides to the patient are included in the hospice rate. In 2019, CMS released a report analyzing 2016 Medicare Part D payments being made for beneficiaries on hospice care. Part D is the Medicare prescription drug plan. The study focused on four categories of drugs that are often prescribed to patients at the end of their lives as well as two disease specific drugs for two diseases. Part D should not pay for drugs if the patient is on hospice and the drug is covered under the hospice benefit. Based upon sample results, CMS estimates that Medicare paid $160.8 million for drugs that hospice agencies should have paid for, constituting and overpayment to hospice.
How can a hospice use this information?
With a better understanding of the underlying motivation for each of these target areas, a hospice agency should carefully look at the data on its PEPPER reports to identify any metrics that indicate a need for further investigation and possible process improvements. These reports are a powerful way to benchmark a hospice agency’s performance relative to itself (over a running three year period) as well as relative to other hospice agencies – across the nation, in its state, and in its MAC jurisdiction.
Where can you get more information?
- Understanding the PEPPER report: Understanding Pepper
- PEPPER Report User Guide: User Guide
- PEPPER Resources: Resources


0 Comments
Trackbacks/Pingbacks