by editor | Nov 13, 2022 | Compliance and Regulatory - Directors, Documentation - Chaplains, Documentation - Nurses, Hospice 101 - Aides, Hospice 101 - Chaplain, Hospice 101 - Nurses, Hospice 101 - Social Workers, Intake, Medical Records, Metrics and KPIs, Rules and Regulations - Chaplains, Rules and Regulations - Nurses, Rules and Regulations - Office Team, Rules and Regulations - Social Workers
HCI is a single comprehensive metric reflecting ten indicators of care delivered during a hospice stay — from admission to discharge. This metric, which is included in the patient Care Compare portal, is intended to provide patients, families, and caregivers with an added metric to support informed healthcare choices.
What are the data sources for this metric?
HCI is calculated from Medicare claims data. A hospice agency does not need to submit any additional data to CMS for the calculation of this metric. The HCI metric captures care processes throughout the duration of a patient’s hospice care – from admission through discharge. Only data for Medicare fee for service patients who have been discharged from hospice is included in the HCI metric. CMS calculates HCI using eight consecutive quarters of data. Hospice agencies with fewer than 20 discharges in the reporting period are not assigned an HCI value. By including eight quarters of data, CMS is expanding the set of hospice agencies for which an HCI value will be reported. CMS will update the HCI metrics once each year.
What does the HCI metric measure?
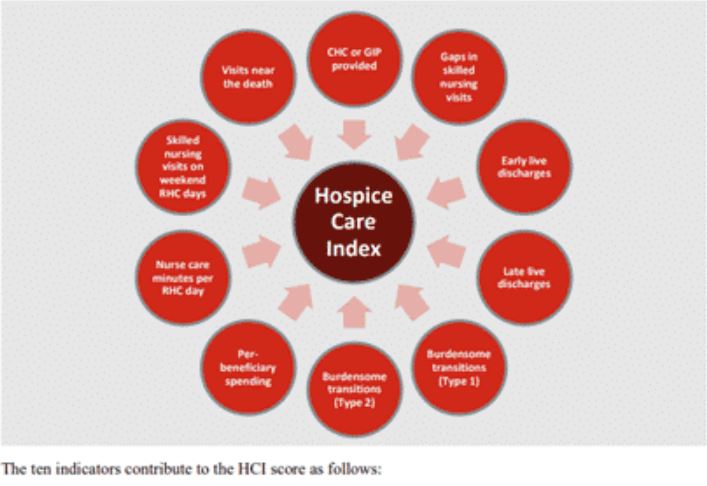
HCI is a single comprehensive metric comprised of the following ten individual indicators of care.
- CHC/GIP provided
- Gaps in skilled nursing visits
- Early live discharges
- Late live discharges
- Burdensome transitions (Type 1)
- Burdensome Transitions (Type 2)
- Per-beneficiary Medicare spending
- Nurse care minutes per routine home care days
- Skilled nursing minutes on weekends
- Visits near death
Each indicator measures a different aspect of hospice care. A set of the HCI indicators measure the agency’s provision of higher level of care as needed and more frequent visits closer to the time of death, as measured by indicators
- Gaps in skilled nursing visits
- Nurse care minutes per routine home care day
- Skilled nursing minutes on weekends
- Visits near death
A set of HCI indicators measure patterns of live discharges and transitions, as measured by indicators
- Discharges from hospice followed by hospitalization and hospice readmission
- Discharge from hospice followed by patient dying in the hospital
- Early live discharges
- Late live discharges
Finally, an HCI indicator is used to measure appropriateness of use of the hospice benefit
- Per beneficiary Medicare spending
Medicare’s overall objectives of the HCI metric are twofold: (i) to ensure that all hospice patients are receiving the care that they need and (ii) to identify indicators of fraud.
How is the HCI metric calculated?
The HCI metric simultaneously monitors all ten indicators of care. The ten indicators are then combined into a single value between zero and ten, where ten is the highest value. Each indicator equally affects the HCI value, reflecting how each aspect of care delivered, from admission to discharge, shares the same level of importance.
Specifically, the hospice agency is awarded one point for each of the ten indicator criteria the agency meets. A hospice receives a point for an indicator if its value exceeds a prescribed threshold. The threshold is determined as a function of the overall values for that indicator across all hospice agencies. The more indicators a hospice agency meets, the higher the agency’s HCI value. The sum of the points earned from meeting the criterion for each indicator yields the agency’s aggregated single HCI value.
When was HCI introduced and where can the metric be viewed?
The HCI metric was added to the HQRP and began public reporting in 2022.
The single aggregate HCI metric can be seen under the Quality of Patient Care section on the Care Compare website.
The details of the HCI metric – including the values for each of the ten individual HCI indicators – can be found in the Provider Data Catalog.
How can a hospice see details about its HCI value?
To support a hospice agency’s quality improvement efforts, CMS shares the details of an agency’s HCI indicator scores in the Hospice Agency Level QM Report in CASPER. An agency can benchmark its indicator values with state and national averages. It can also trend its performance in each indicator over time.
Where can you learn more?
Image from Home Care Pulse
by editor | Sep 20, 2022 | Billing, Billing - General, Compliance and Regulatory - Directors, Financials, Intake, Notice of Election, Rules and Regulations - Nurses, Rules and Regulations - Office Team
by editor | Sep 15, 2022 | Accounts Payable, Billing, Billing - General, Compliance and Regulatory - Directors, Documentation - Nurses, Hospice 101 - Aides, Hospice 101 - Chaplain, Hospice 101 - Nurses, Hospice 101 - Office Team, Hospice 101 - Social Workers, Human Resources, Intake, Medical Records, Metrics and KPIs, Office Setup, Payroll, Rules and Regulations - Chaplains, Rules and Regulations - Nurses, Rules and Regulations - Social Workers, Rules and Regulations - Volunteers
Are you confused by the Acronym Alphabet Soup?
Does the never ending list of acronyms used in the hospice and healthcare industry leave you confused?
Are you worried that you may confuse CMN with CMP?
To help sort out the confusion, we add here links to lists of acronyms:
Use these acronym listings to help clarify things when you inevitably are faced with acronym confusion!


by editor | Sep 12, 2022 | Billing, Billing - General, Compliance and Regulatory - Directors, Documentation - Nurses, Financials, Intake, Medical Records, Notice of Election
The Notice of Election (NOE) is more than a clinical administrative task; it is a critical financial trigger. In the hospice revenue cycle, the NOE serves as the formal notification to Medicare that an agency has assumed responsibility for a patient’s care. Failure to file this document within the mandatory window results in permanent, unrecoverable revenue loss.
The Standard for Timely Filing
Medicare regulations require that an NOE be filed within five calendar days after the beneficiary’s hospice admission date. For a filing to be considered legally “timely,” it must meet two specific criteria:
- Receipt Date: The NOE must be received by the Medicare contractor within five calendar days after the admission date.
- Processing Status: The NOE must successfully process and reach the final status/location P B9997.
The Cost of Non-Compliance
When an NOE is filed late, the financial consequences are immediate. Medicare will not reimburse the agency for the days of care provided from the date of admission until the date the NOE is finally submitted and accepted.
Consider this example of a late filing:
- Admission Date: May 1st
- NOE Receipt Date: May 10th
- The Result: The agency is responsible for the cost of care from May 1st through May 9th. These nine days are considered “non-covered” and represent a 100% loss of revenue for that period.
The “RTP” Trap: Resubmissions and Timeliness
One of the most common drivers of revenue loss is the Return to Provider (RTP) error. If an NOE is submitted within the five-day window but contains errors, it will be sent back for corrections.
It is critical to understand that the resubmission date becomes the new “receipt date” for timeliness purposes. Even if your initial attempt was on day two, if the corrected version isn’t accepted until day ten, the entire period remains non-covered. This is why “clean” initial submissions are just as important as “fast” submissions.
Operational Requirements for Late Filings
If an agency identifies that an NOE was filed untimely, the subsequent claim must be coded specifically to reflect the non-covered period. This is not optional; failure to code correctly can lead to claim rejections or audits.
- Occurrence Span Code (OSC) 77: This must be used on the claim to identify the specific dates that are non-covered due to the late NOE.
- Dual-Line Billing: The claim must be split into two distinct rows: one for the non-covered days (associated with OSC 77) and one for the covered days following the NOE acceptance.
Leadership Strategy: Moving to a 48-Hour Standard
To eliminate the risk of late filings, high-performing agencies do not aim for the five-day deadline. Instead, they implement an internal 48-hour submission rule.
By requiring NOEs to be filed within two days of admission, leadership creates a “buffer” to handle unexpected RTP errors or technical issues with the billing software. This proactive operating rhythm ensures that administrative delays never compromise the agency’s financial stability or the clinical team’s ability to focus on patient care.
by editor | Sep 8, 2022 | Billing, Billing - General, Compliance and Regulatory - Directors, Intake, Notice of Election, Rules and Regulations - Nurses
What is a Notice of Election?
When a Medicare beneficiary elects hospice services, the hospice must complete an election notice with the beneficiary and file a Notice of Election (NOE) with Medicare. A Notice of Election (NOE) is the formal mechanism used to notify Medicare that a beneficiary has elected the hospice benefit. While the concept is straightforward, the submission process requires high technical accuracy to meet the mandatory five-day filing window.
Submission Timing and the “Clean Claim” Requirement
Medicare requires that an NOE be submitted and processed before the agency files its first claim for that beneficiary. Since October 1, 2014, the standard has been strict: the NOE must be filed within five calendar days of the election date.
To satisfy this requirement, the submission must be “clean” – meaning, it is free of data entry errors. If an NOE contains errors, it is Returned to Provider (RTP). Once corrected and resubmitted, the NOE receives a new receipt date, which can push the filing outside the five-day window and result in non-covered days.
Three Methods for NOE Submission
Hospice providers currently have three avenues for submitting the NOE. Each carries different levels of administrative burden and risk of error.
1. Electronic Data Interchange (EDI) – Recommended
Effective January 1, 2018, Medicare allowed for NOE submission via EDI. This is the most efficient method for agencies seeking a predictable operating rhythm.
- The Benefit: Data is exported directly from the patient’s Electronic Medical Record (EMR), virtually eliminating manual keying errors.
- Operational Note: NOEs submitted via EDI should not be batched with standard claims; they must be processed as distinct transactions.
2. Direct Data Entry (DDE)
DDE involves manually entering the NOE into the Fiscal Intermediary Shared System (FISS).
- The Benefit: DDE provides real-time access to monitor claim status, check beneficiary eligibility, and correct errors.
- The Risk: Because this requires manual entry across multiple screens, it is highly susceptible to human error, which often leads to RTP status and potential filing delays.
3. Paper Submission (UB-04)
While technically permitted, submitting a physical UB-04 form via mail is the least efficient method.
- The Risk: This method is subject to mail delays and manual processing times at the Medicare Administrative Contractor (MAC), making it nearly impossible to guarantee compliance with the five-day window.
Ensuring Submission Accuracy
Regardless of the method chosen, the data requirements remain the same. Leadership should ensure that the billing team is utilizing verified “job aids” from their specific MAC (such as Palmetto GBA, CGS, or NGS) to ensure every data field – from the NPI to the admission date – is perfectly aligned with the election statement.
By prioritizing EDI submission, agencies can reduce their reliance on manual intervention and ensure that the “engine” of the revenue cycle remains stable and compliant.

by editor | Aug 4, 2022 | Billing, Billing - General, Compliance and Regulatory, Compliance and Regulatory - Directors, Documentation - Nurses, Financials, Intake, Patient Care, Rules and Regulations - Nurses, Rules and Regulations - Office Team
Prior to the third hospice benefit period, and prior to each subsequent benefit period, a hospice physician or nurse practitioner is required to have a face to face encounter with the hospice patient to recertify that the patient continues to be Medicare eligible for hospice benefits. The face to face encounter must occur within 30 calendar days prior to the start of the third benefit period and each subsequent benefit period.
The face to face encounter is necessary to recertify that the patient remains eligible for Medicare hospice benefits. If face to face encounters are not performed timely, the patient is is no longer hospice eligible. The hospice may continue to provide hospice services to the patient but may no longer continue to bill Medicare. Instead, the hospice would need to assume all financial responsibility for the patient until such time that the hospice is able to reestablish patient hospice eligibility. The patient may be readmitted to hospice once hospice eligibility criteria are once again met.
What if there are exceptional circumstances that cause the hospice to be unable to timely complete the face to face encounter?
What are exceptional circumstances?
If a patient is admitted and is in the third benefit period or later, the hospice agency may be unable to perform the face to face encounter prior to the start of the benefit period.
For example, if the patient is an emergency weekend admission and the nurse practitioner or hospice physician is unable to meet with the patient prior to hospice admission. The patient is only seen the following Monday.
Another exceptional circumstance may be where the CMS data system is unavailable and the hospice agency is unaware that the patient is in the third or later benefit period.
In these documented exceptional circumstances, the face to face encounter is considered timely if it is completed within two days after admission.
In addition, if the patient dies within two days of admission, the face to face encounter is considered complete.
Where can you get more information?
Details on Medicare Face to Face encounter requirements: Medicare F2F encounter requirements
