A hospice face to face encounter is a step in patient recertification beginning with the third benefit period and each benefit period thereafter. The goal of hospice face to face patient encounter is to encourage greater involvement of the physician in the care of patients who have been on hospice for an extended period of time. These patients will require a face to face visit from the physician or from a hospice nurse practitioner who will determine continued hospice eligibility. The face to face encounter is one part of hospice recertification. As such, the face to face encounter will also occur prior to recertification.
When must a face to face encounter take place?
A face to face encounter must take place within 30 days prior to the start of the patient’s third benefit period. It also must take place within 30 days prior to each subsequent benefit period. The requirement for a face to face encounter considers the patient’s hospice stays across all hospices. For example, if a patient spent 100 days at Hospice Agency A and then switched to Hospice Agency B, Hospice Agency B will need to conduct a face to face encounter within 50-80 days of the patient’s admission. That is, when the patient is admitted to hospice B the days of counting toward the face to face encounter begin from the first day that the patient entered any hospice care.
How will I know if the patient has had prior hospice care?
Upon admitting a patient, the hospice agency should check the Common Working File to determine the patient benefit period and whether a face to face encounter is required.
Who may conduct the face to face encounter?
Either the hospice physician or nurse practitioner (NP) may conduct the face to face encounter. The hospice physician may be an employee or contracted by the hospice agency. If the NP conducts the face to face encounter, the NP must be an employee of the hospice and is not permitted to be a contractor (since nursing is a core service).
What should the recertification narrative include?
The third benefit recertification – and each subsequent recertification – will need to contain clinical findings that support continued hospice eligibility. The narrative must include an explanation of why the clinical findings support a life expectancy of six months or less.
If the physician conducts the face to face, he or she will be responsible to write the narrative about the clinical findings regarding the patient’s condition and for certifying the patient’s continued eligibility for hospice.
If the nurse practitioner conducts the face to face encounter, he or she will report back the clinical findings to the interdisciplinary team as well as to the hospice physician who will certify as to whether the patient is eligible for continued hospice care.
The recertification requires an attestation
The clinician who conducts the face to face encounter must attest in writing that the face to face encounter was performed with the patient and must include the date that the encounter occurred.
If an NP conducts the encounter, the NP must attest that the clinical findings were sent to the certifying physician.
The attestation is signed and dated in is included as a separate and distinct section of the recertification. The recertification also clearly notes the benefit period dates for which the recertification applies.
What happens if the face to face does not take place timely?
If the face to face does not take place, the patient is considered no longer considered terminally ill and therefore is not eligible for the Medicare hospice benefit. The patient remains ineligible until such time that the face to face encounter occurs and it is confirmed that the patient is once again hospice eligible. The patient must be discharged from the hospice but can be readmitted once the face to face encounter occurs. Medicare does permit the hospice agency to continue to provide services at the agency’s expense until the patient’s eligibility is reestablished. However, this care will be provided outside of the Medicare hospice benefit.
Hospice Conditions of Participation – employees versus contractors
Hospice conditions of participation require that almost all hospice core services are delivered by hospice agency employees and may not be delivered by contractors. Hospice core services include:
Nursing services
Social services
Counseling services including spiritual, bereavement and dietary
Physician services
Although physician services are a core service, the regulations permit a hospice agency to contract for physician services.
When may a hospice use contracted staff for core services?
Other than physician services, only under extraordinary circumstances may a hospice agency use contracted staff for core services.
What are extraordinary circumstances?
Under extraordinary circumstances, a hospice may use contracted staff to provide core services. Examples include:
Patient needs unexpectedly exceed the capacity of hospice agency employees, due to unanticipated surge in demand. In this case, contracted staff may be temporarily used to service patients.
Temporary staffing shortages, for example due to illness, result in the inability of the hospice to service patient needs. In this case contracted staff may be used to temporarily supplement hospice agency employees.
A hospice patient travels outside of the hospice agency’s service area. In this case the agency is permitted to contract with another Medicare certified hospice agency to provide services to the patient while the patient is traveling.
What is hospice initial accreditation and why is it important?
Hospice initial accreditation is a way to ensure delivery of consistent and high quality services across all accredited hospice agencies. The accreditation program ensures that the hospice agency is fully compliant with Medicare Conditions of Participation. The program also reviews that the hospice is compliant with state and local laws. An on-site survey conducted by the accrediting organization evaluates the quality of the clinical care provided, quality and compliance of patient records, policies and procedures, and performance improvement. Patient and family experiences and quality outcomes are also reviewed. The organization’s financial and long term viability is also studied via review of budgets and other related metrics.
When would a hospice want to complete the accreditation process?
A home hospice must complete the initial Medicare accreditation process before it is able to bill Medicare for services provided to patients. CMS has approved three accrediting organizations (AO) to conduct Medicare surveys and accreditation for hospice agencies: CHAP, ACHC, and JCAHO. These agencies have standardized accreditation and assessment processes although the requirements and actual on-site survey review may vary depending upon state and local regulations.
There are six key elements of the initial accreditation process
File and obtain state home licensure
Register with accreditation organization
Obtain CMS 855A
Develop patient caseload – verify agency is meeting Conditions of Participation
Ensure Conditions of Participation are being met
On-site survey visit
We now discuss each of these elements in greater detail.
Element 1: The process begins with the hospice filing a state home hospice licensure. Each state has its own requirements for approval. So this process and its time lines will differ by state.
Element 2: Register with one of the three accreditation organizations (AO). The AO will require a registration fee. Although the accreditation will be received from CMS, Medicare has granted authorization to AO to conduct the accreditation process on behalf of CMS. The AOs have local branches, allowing them to customize their surveys for state and local regulatory requirements.
Element 3: Confirm 855A is accepted by the Medicare Administrative Contractor (MAC) that is appropriate for the hospice agency’s region: Palmetto GBA, NGS or CGS.
Element 4: Develop patient caseload. Specifically, the hospice must have serviced five patients, with at least three active at the time that the AO conducts the survey. Further, although the hospice is not currently billing Medicare, all patients must be treated as if they are Medicare eligible. All documentation must be completed within the Medicare required time frames and services must be provided by employees, as per Medicare guidelines.
Element 5: Ensure Conditions of Participation are being met. This element involves a number of different items.
The first item is that the hospice agency must verify it is providing all core services using hospice agency employees. Core services include nursing, social work, and counseling including spiritual, bereavement, and dietician. These services must be provided using hospice employees. Contractors may not be used to provide these services. Physician is also a core service but CMS permits the medical director and alternate medical director services to be provided using either hospice agency employees or contracted services.
The second item is to very that the hospice agency is able to provide all non core services using either hospice agency employees or contractors. Non core services include the therapies: physical therapy, occupational therapy, and speech therapy. Additionally, the agency must verify that it is able to provide aide services. It also must be able to demonstrate that it has a bereavement program, even if this service is not yet being used.
The third element is that the hospice agency must verify it can provide all four levels of care including routine, GIP, respite, and continuous care. Not all of these levels of care must be provided through hospice employees; the agency may contract to provide these levels of care.
As a final element, the hospice agency should demonstrate that it can provide DME, pharmaceuticals, drugs and biologicals.
Element 6: On-site survey. Once the hospice confirms that that prior five elements are completed, it will indicate to the AO that it is ready for a Site Visit. The date of the Site Visit will not be announced to the hospice agency but will typically occur within 45 days of when the hospice agency indicates site readiness. The survey will be conducted on-site over three consecutive days. The AO will review patient medical records, accompany staff on patient home visits, and review both clinical and non-clinical hospice agency policies and procedures. The AO will also review the agency for financial viability by reviewing budgets and other related metrics.
What happens after the survey is completed?
After the AO completes the on-site survey, the hospice agency will be notified of the final findings of the survey. There are four possible outcomes.
Agency passed with no deficiencies
Agency passed with minor deficiencies; agency must write an action plan that must be accepted by the accrediting organization
Agency has major deficiencies; deficiencies must be resolved, followed by another three day survey
Agency failed the survey; agency must restart the entire process
What happens after a hospice agency is issued its accreditation letter?
The AO sends a copy of the accreditation letter to the state department of health. Upon receipt, the state will confirm that the agency continues to meet all state requirements for Medicare eligibility. CMS will also contact the Fiscal Intermediary to confirm that the agency is located and operating at the physical address indicated on the Medicare application. The hospice agency will then be issued a Provider Number, also referred to as CMS Certification Number (CCN).
In order to bill Medicare, the hospice agency must enroll in EDI and will be issued a Billing Number. We discuss this process separately.
Where can you find more information?
This video from ACHC provides a description of the initial hospice accreditation process
A payer is the company of government agency that pays the provider, i.e., the hospice agency, for the medical service that is administered to the patient.
For most hospice agencies, Medicare is the primary payer for hospice services. See, for example, this study published by Bazell et al., 2019, https://bit.ly/3RS805r. The characteristics of payment vary by payer. As such, an agency should understand the distribution of its revenues and receivables across different payers. In addition to understanding the breakdown of total receivables, the agency should look at distribution of receivables by payer – further broken down by aging bucket.
Expected time to be paid on a claim varies by payer. For example, payment for a Medicare claim is usually received within 14 days of the date the claim is submitted. A claim submitted to a commercial payer will take longer and further varies by the commercial payer. It is important to monitor time until payment is received for each payer. Delay in payment is an opportunity to quickly identify if there is a billing error that needs to be corrected. Or, there may be an opportunity to improve the billing and collection process that will result in an increase in speed of collections.
It is also useful to compare your agency’s metrics to industry standards. Metrics that are worse than industry standards could point to areas of the collections process that could benefit from process improvement.
Aging Accounts Receivables for Medicare and Commercial Payers
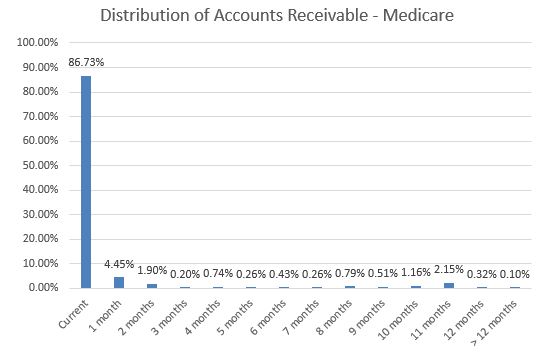
The following graph shows aging accounts receivable for the Medicare payer. As we see from the graph, over 90% of the receivables are less than two months old.
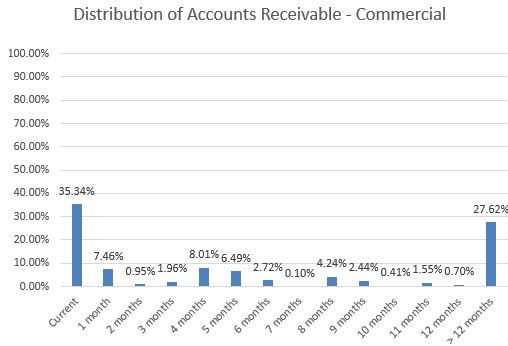
In contrast, here we can see the distribution of aging accounts receivable for commercial payers for the same hospice agency.
In contrast to the Medicare accounts receivables, here only 43% of the receivables are less than two months old. 25% of the receivables are between four and eight months old. More significantly, more than 25% of the outstanding receivables are more than 12 months old – a sign that there may be a high number of receivables that may have to be written off.
What is the key takeaway?
Different payers have different payment patters and different rules for timely submission of claims. Hospice agencies need to have a good understanding of the distribution of their claims and the distribution of their outstanding accounts receivable to reduce the likelihood of write-offs.
The age of accounts receivable (AR) is the time that has elapsed from the time the agency delivered the service to the patient until current date. Aging AR is typically grouped into monthly buckets (e.g., 0-30 days, 31-60 days, etc.). Total dollar value of outstanding (aging) AR should be monitored each month, grouped by monthly buckets.
Consider the aging AR in the graph above. The horizontal axis shows different buckets of AR, where Medicare is the payer. “Current” represents dollars outstanding for services rendered within the most recent 30 days. “1 month” is dollars outstanding for services rendered in the most recent 31-60 days, etc. The vertical axis represents the percentage of the total Medicare dollar amounts of AR in each of the aging buckets.
How is the Accounts Receivable Distributed over Aging Buckets?
The high dollar amounts in the the first AR bucket followed by a drastic drop in outstanding AR is typical for the Medicare payer. Most agencies bill on a regular cycle (biweekly or monthly) so the large volume of outstanding AR in the “Current” bucket is mostly comprised of services that have not yet been billed out or have just been billed out to Medicare.
The outstanding AR drops but remains elevated in the “1 month” bucket. The agency is waiting to collect on services for which it has billed. It takes approximately 14 days to receive payment from Medicare. Aging AR is low in all remaining aging buckets. This is because the agency has billed and collected for most of its Medicare AR services.
What is Medicare Timely Filing?
Medicare claims must be filed no later than 12 months from the date services were provided. This includes resubmitting corrected claims that were unable to be processed. Again considering the aging AR in the graph above, note the volume of AR in the 10 month and 11 month aging buckets. AR in these aging buckets may be approaching Medicare’s timely filing deadline. Any claims in these buckets that have not yet been billed to Medicare will be not be able to be billed due to timely filing. The agency should quickly investigate the AR in these buckets.
Most agencies have a greater than 99% collection rate for Medicare AR. There should not be significant Medicare AR that is uncollectible.
In addition to monitoring total dollar value of aging AR, there are other useful classifications and breakdowns of aging AR that should be monitored on a monthly or even weekly basis.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga_
ID used to identify users
2 years
_gid
ID used to identify users for 24 hours after last activity
24 hours
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.