Documentation is an essential part of patient care, especially when you are working as a member of a hospice team. Hospice documentation involves writing down everything you did, observed, and discussed with the patient and their family during your visit. This includes the care you provided, any changes in the patient’s health, and specific events that could impact the patient’s future health. Documentation is like a diary that keeps track of the patient’s journey, making sure everyone involved in the patient’s care is on the same page.
Why is documentation important?
Documentation is a way for the team members to share information about the patient’s health condition and any changes in the patient’s condition. It also serves as legal proof of the care that was provided to the patient. More specifically, there are a number of reasons why documentation is important:
Communication with the care team: Since hospice care involves multiple healthcare professionals, documentation helps everyone stay informed. Not all members of the care team are present during each patient visit. Notes in the medical record provide vital updates on the patient’s condition and ensure that all members of the care team know how the patient is doing and can make informed decisions about patient care based upon the most up-to-date information about the patient’s health status.
Legal requirements: Documentation is also a legal requirement. Documentation serves as proof that a patient visit occurred and that specific care was provided. If something goes wrong or if there is a legal question about the patient’s care, the notes in the patient’s medical record can be used to show what happened and when.
Continuity of care: Proper documentation ensures that the care plan is followed consistently. It helps the team track the patient’s progress and make any changes to the patient’s care, as needed. Without accurate records, important details may be missed which can lead to gaps in the patient’s care.
Guidelines for good documentation
As we have discussed, documentation plays a critical role in helping with communication between the members of the care team, helping meet legal requirements, and in ensuring continuity of patient care. So how can you make sure that the documentation that you write is good documentation — that it is clear, accurate, and useful? The following are some guidelines to follow:
Document right after the visit: Document your visit immediately after you complete your visit. This helps you remember exactly what happened and ensures that your notes are fresh and accurate.
Be clear: Think about what you want to write before you start. Make sure your notes are easy for other members of the care team to understand. Write your notes in a way that it is easy to follow, so that others can quickly find the information that they need.
Stick to the facts: Only write down what actually happened. Avoid including your opinions or assumptions.
Use quotation marks: If a patient or family member says something important, include their exact words in quotation marks. This helps convey the exact message they intended.
List your tasks: Write down any tasks you did, helped with, or observed.
Be specific: Include specific information to help other members of the care team better understand the patient’s current condition. Examples of specific details are (depending on role):
Patient’s mood
Any pain or changes in pain
How well patient moved around
Changes in appetite
Weight changes
Changes in need for oxygen
Increased or decreased difficulty breathing
Conclusion
Good documentation is more than just writing things down. It is a vital part of providing high quality care. By keeping accurate, detailed, and timely records you help ensure that the patient receives the best possible care and you fulfill your legal responsibilities as a healthcare provider. When in doubt, always ask for help to make sure that your documentation is accurate and useful. Your supervisor, clinical director, or members of your QAPI team are all great resources in case you have questions.
Root Cause Analysis (RCA) is a systematic and structured process used to identify the root causes that results in an undesirable outcome or adverse event and to develop corrective actions. The goal of RCA is not just to treat the symptoms of a problem but to delve into the underlying causes of the failure. By understanding these causes, a hospice agency can develop strategies to mitigate risks and implement corrective actions to prevent future occurrences. This approach to addressing adverse events will lead to improved patient safety and enhanced quality of care. Further, by promoting a culture of safety, RCA fosters a culture of transparency, accountability, and continuous improvement in the hospice agency.
When is root cause analysis used
A hospice agency can use root cause analysis to investigate any unexpected occurrences such as hospice acquired pressure ulcers, medication errors, or process variations where recurrence could result in serious adverse outcomes. Candidates for RCA may be identified via patient satisfaction surveys, incident reports, surveys, or other reports and audit activities. A root cause analysis focuses on systems and processes, rather than individuals in the agency. The objective of the RCA is to reduce the risk of recurrence by identifying opportunities to improve or redesign systems or processes. By implementing system changes, this will lead to sustained system improvement.
Elements of root cause analysis
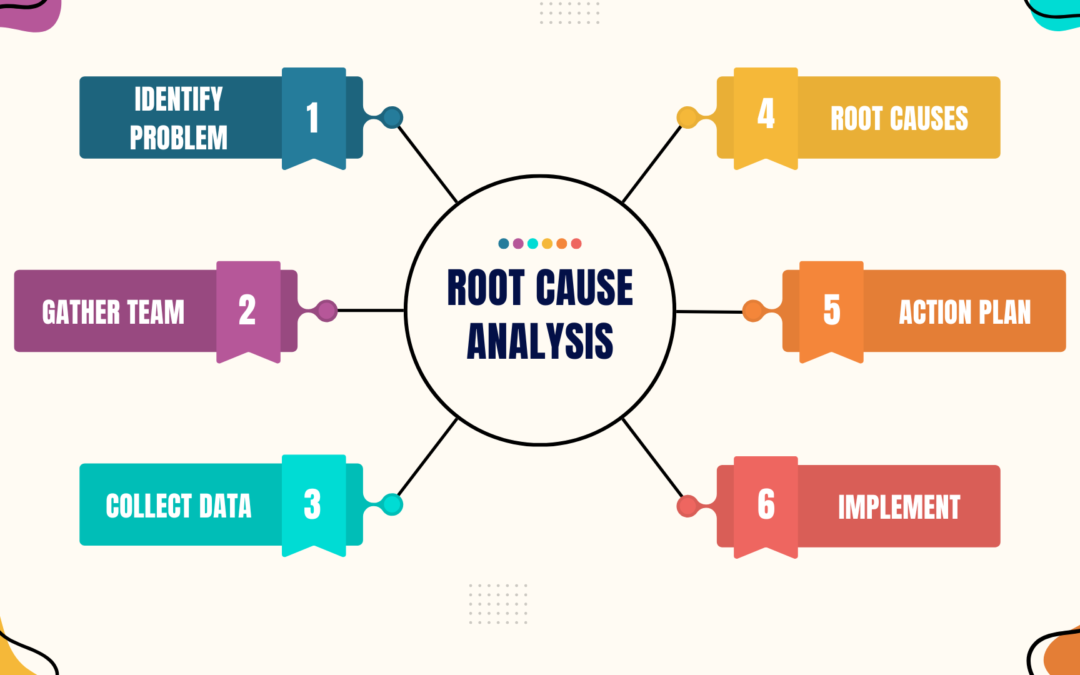
A comprehensive root cause analysis includes the following elements:
Problem identification: Identify the adverse event to be investigated and gather preliminary information. Events and issues can come from many sources such as patients and their families, staff, or regulatory bodies. The agency should have a process for deciding what events are selected for RCA.
Define the event: Clearly describe the adverse event, error, or near miss. Include specifics such as what happened, where, when, and who was involved.
Gather initial data: Collect all relevant information about the event including incident reports, patient records, and witness statements.
Assemble RCA team: Select the members of the RCA team and the team facilitator. Team members should be knowledgeable about the processes and systems that they will be investigating.
Multidisciplinary team: Form a team that includes individuals with diverse expertise and perspectives. This may include clinicians, administrators, and support staff.
Assign roles and responsibilities: Clearly define the roles and responsibilities of each team member to ensure an organized and effective RCA process.
Data collection and investigation: Collect and organize the facts about the adverse event that will be investigated.
Detailed event timeline: Create a detailed timeline of events leading up to, during, and after the incident. This helps in understanding the sequence of events.
Conduct interviews: Interview staff involved in the event to gain insights into what happened and why. Ensure a non-punitive approach to encourage open and honest communication. Review documentation: Examine all relevant documentation including patient records, policy and procedure manuals, and any relevant logs.
Identify contributing factors and root causes: Identify the situation, circumstances, or conditions that increased the likelihood of the adverse event. Conduct a thorough analysis of contributing factors that lead to identification of underlying process and system issues.
Cause and effect analysis: Use tools such as fishbone diagrams (Ishikawa) or flow charts to map out the possible causes and identify the root causes. Five whys technique: Ask “why” repeatedly (usually five times) to drill down to the underlying root cause(s) of the problem.
Develop action plan: Develop plan for best changing the processes and systems to reduce the likelihood of another similar event. Design and implement changes to eliminate the root causes. This may involve creating new processes.
Corrective actions: Develop specific, measurable, achievable, relevant, and timebound (SMART) corrective actions to address the root causes.
Assign responsibility: Assign responsibility for implementing each corrective action to specific individuals or teams. Timeline: Establish a timeline for the implementation of each corrective action
Implementation and Monitoring: Implement the plan and evaluate its performance. Create mechanisms to gather data that can be used to measure the success of changes that were introduced.
Implement changes: Put the corrective actions into practice. Ensure that staff are trained and aware of changes to procedures or policies. Monitor effectiveness: Continuously monitor the effectiveness of the corrective actions. This may involve regular audits, follow up assessments, and a feedback mechanism.
Documentation and Reporting: Create documentation of the RCA process including all findings, root causes, and corrective actions taken. Share findings with stakeholders, promoting a culture of transparency.
Detailed Reports: Document the entire RCA process, including findings, root causes, corrective actions, and implementation outcomes.
Communicate findings: Share the RCA findings and action plans with all stakeholders including staff, patients, and regulatory bodies.
Continuous improvement: Review the RCA process on a periodic basis to identify any necessary modifications or areas that could benefit from improvement. Continuous improvement ensures that the agency promotes a culture of growth and continuous learning.
Review and revise: periodically review the RCA process and outcomes to ensure sustained improvements. Revise strategies as necessary based on new data and feedback.
Promote a learning culture: Foster an environment where continuous learning and improvement are encouraged and staff feel empowered to report issues and participate in problem solving.
Root cause analysis is a vital tool in hospice care for understanding and addressing the underlying causes of adverse events and errors. By systematically identifying and correcting these root causes, hospice agencies can significantly enhance patient safety, improve quality of care, and promote a culture of continuous improvement. A well-executed RCA resolves the immediate issue and provides valuable insights to prevent future occurrences, thereby ensuring better outcomes for patients and their families.
In accordance with the Conditions of Participation, a Medicare certified hospice agency must have a governing body. The governing body has ultimate responsibility for the hospice agency, including legal and financial authority. Medicare Conditions of Participation require that the governing body is informed of the ongoing activities at the hospice agency, including patient care delivery issues and all QAPI activities. The governing body must also appoint a qualified hospice administrator – a hospice employee with the necessary education and experience – who is responsible for hospice daily operations.
The governing body must meet at least quarterly and must maintain written minutes of its meetings.
There are two Conditions of Participation – 418.100 and 418.58 – that relate to the hospice governing body.
Condition of Participation 418.100
This Condition of Participation defines a standard that the governing body is responsible for management of the hospice agency, including its fiscal operations, provision of services, and continuous quality assessment and performance improvement (QAPI) efforts. The governing body also assumes full legal authority of all hospice operations. It further specifies that the governing body should appoint an administrator that reports to the governing body and who is responsible for hospice agency daily operations. The hospice administrator must be a hospice employee and must have necessary training, education, and experience. CMS does not specify the process by which an administrator should be selected by the governing body. If a hospice agency has multiple locations, the governing body is responsible for administration, supervision, and services for all locations as well as for any arranged services.
Condition of Participation 418.58
This Condition of Participation discusses requirements of a hospice agency’s QAPI program. The governing body must ensure that the hospice agency maintains and implements an ongoing quality improvement and patient safety program. Program performance must be monitored on a regular basis. Further, the governing body must ensure that one or more individuals are selected to lead the organization’s QAPI efforts.
The hospice agency’s organization documents must specify that the hospice governing body is responsible for the QAPI program. Additionally, the governing body specifies the frequency of data collection and level of detail of data collected by the QAPI program.
Are there any state regulations?
State hospice licensure regulations may impose additional requirements on the hospice governing body. They may also have specific requirements on the administrator that is selected by the governing body. A hospice is required to meet the most stringent requirements (whether state or federal).
Surveyors will check that all conditions are met. A hospice agency should maintain evidence of the governing body’s role and activities. Governing body authorizations and activities should be documented in governing body meeting minutes, company organization documents, and company policies and procedures.