
by editor | Apr 15, 2026 | Grief & Loss - Social Workers, Grief and Loss, Keys to Compassionate Care, Resources and Readings
Supporting grief in children is a fundamental part of the hospice mission. Hospice clinicians often observe well-meaning adults trying to shield children from the reality of mortality. Their aim is to preserve a sense of “childhood innocence”. However, a 2026 narrative review highlights that death is a persistent presence in our lives, and even very young children are naturally curious about it. While adults often avoid these conversations because they feel “unqualified” or personally uncomfortable, children actively want to discuss and understand dying. This avoidance is often rooted in what Ernest Becker famously described as the “denial of death” – a cultural stigma that prevents us from integrating mortality into our educational and family lives. When we stay silent, we don’t actually protect children. Instead, we leave them alone to make sense of life’s biggest and most confusing questions.
The Seven Building Blocks of Understanding
A child’s grasp of death isn’t a single “aha” moment. Rather, it is a gradual process of piecing together seven different building blocks. This developmental journey was famously explored by researchers like Maria Nagy and Jean Piaget, who noted that children’s ideas about death mature alongside their cognitive abilities. According to the Jean Piaget Society, children are active participants in building their own understanding of the world. What this means is that children don’t just “soak up” information. They work hard to make sense of it. By the age of 12, most children understand the three core facts: that the body stops working (biological cessation), that you cannot come back to life (irreversibility), and that it happens to every living thing (universality). However, modern research highlights four other critical areas children navigate:
- Causality: Understanding that death always has a specific cause, such as illness or an accident.
- Applicability: Recognizing that only living things can die.
- Personal Mortality: Realizing that they are personally included in the rule of death.
- Noncorporeal Speculation: Wondering about what happens beyond the physical world, such as an afterlife.
The Media Gap: Why Disney Isn’t Always the Best Teacher
If adults refuse to talk about death, children often turn to media for answers. Recent studies, such as the one conducted by Bridgewater et al. (2021), have found that children are often introduced to death through animated films long before they ever discuss it with an adult. This can be clinically problematic because many movies portray death as something that only happens to “villains,” while “heroes” are often magically brought back to life. As research by Graham et al. (2018) suggests, this “cartoon logic” can leave a child incredibly confused when a real-world loved one dies. They may struggle to understand why their “good” family member can’t come back, or worse, they may wonder if the death is a punishment for being “bad”. This guide is designed to support the hospice community in replacing these confusing myths with gentle, consistent, and accurate truths.
Opening the Door: Reframing the Hospice Conversation
To foster a healthy understanding, we must guide families toward clear and direct communication. This means avoiding common euphemisms like “passed away” or “went to sleep,” which can be easily misinterpreted by a child’s literal mind. When a child initiates a conversation – which is how these discussions often begin – adults frequently react with shock or discomfort. This reaction can invalidate the child’s curiosity and make them feel that wondering about death is “wrong”. Instead, we should encourage parents to meet these blunt questions with validation and factual honesty, treating death as a natural extension of biology and the world around us.
Practical Tools: Preparing Children Before a Loss
Preparing a child for death is most effective when it starts before a crisis occurs. One powerful method is using specialized literature that addresses both the biological and emotional sides of death. For instance, books that explain the physical process of the body ceasing to function or the natural process of decay, such as Lifetimes or The Dead Bird, can help explain “biological cessation”. Other resources, like When Dinosaurs Die, offer a straightforward guide to the customs following a loss. To help children navigate “noncorporeal speculation” – the big questions about how we stay connected to those we love even after they are gone – a resource like The Invisible String can be invaluable. Research suggests that these indirect experiences, when guided by a supportive adult, help children build a healthy and coherent framework for death at their own pace.
A Creative Path Toward Resilience
Finally, we can restructure bereavement support through a “pedagogy of death” – an intentional way of teaching children about life’s end. The 2026 review suggests that combining arts-based activities with “philosophical inquiry” is a powerhouse for young minds. This approach, often called Arts-Based Existential Intervention (ABEI), uses drawing or painting to give children a non-verbal outlet for feelings they don’t yet have the words to describe. When we pair that art with guided conversations using the Philosophy for Children (P4C) method, we help them find personal meaning in the face of loss. By moving away from avoidance and toward honest, creative engagement, we can support the psychological well-being and resilience of the youngest members of the families we serve.
The Social Worker’s Toolkit
Recommended Literature
- Lifetimes – Best for explaining the natural “time” of all living things.
- When Dinosaurs Die – A straightforward guide to customs and “what happens.”
- The Invisible String – Excellent for addressing the emotional anxiety of separation.
- The Dead Bird – A gentle look at the physical reality of death through nature.
Clinical Organizations and Activities
References and Further Reading

by editor | Mar 30, 2026 | Blog, Keys to Compassionate Care, Resources and Readings, Resources and Readings
A recent study published in The Journals of Gerontology explores how marital status and social networks impact the quality of end-of-life care for older adults in the United States. Using data from the National Health and Aging Trends Study (NHATS), researchers analyzed ten dimensions of care. Three of these ten dimensions included pain management, respectful treatment, and care coordination. The findings suggest that while many older adults receive high-quality care, certain groups – particularly those who are divorced – face significant disadvantages in their final weeks of life.
Key Conclusions on Social Ties and Care Quality
The research highlights that divorced decedents fared the worst across multiple outcomes. They were less likely to receive “excellent” overall care. They also often struggled to have their personal care needs met or receive respectful treatment. Interestingly, never-married individuals often fared as well as married couples. This is likely due to their proactive nature in building alternative support networks and enlisting paid professional help. Additionally, while spouses remain the primary advocates, siblings and larger social networks were shown to provide superior protection. This is specifically the case for pain management.
What This Means for Hospice and Palliative Care
These findings serve as a wake-up call for those working in long-term care and hospice. Clinicians often operate under the assumption that “family” will naturally step in to fill the gaps in advocacy and care. However, as the American demographic shifts toward more divorced and “kinless” seniors, our standard models of family-oriented care must evolve. We cannot ignore the “advocacy gap” that exists for patients who lack a traditional spouse or child to navigate the complexities of a medical system.
Actionable Takeaways for Healthcare Professionals
What is the immediate takeaway for practitioners? Patients with limited traditional social ties require earlier and more intensive intervention. A patient’s social network must be carefully considered when discussing advanced care planning. Dying patients need help identifying “significant others” – whether they are siblings, friends, or paid caregivers – who can serve as effective “decision partners“. Investing in nurse advocates and social workers is not just a luxury. Every patient, regardless of their marital history, must be treated with the dignity and respect they deserve.
Understanding the Evolving “Good Death”
The concept of a “good death” is increasingly being viewed through a relational lens, where the quality of the experience depends heavily on a patient’s support system. As the number of older adults living without traditional family ties continues to rise, the industry is gaining a clearer picture of how social isolation impacts end-of-life outcomes. Moving forward, many providers remain focused on ensuring that care quality is driven by clinical and personal needs rather than a patient’s marital or legal status.
Strategic Takeaways for the Industry
Recognizing these social shifts allows for a more tailored approach to patient care. Early screening for social vulnerability allows care teams to better identify which patients might need additional support, including nurse advocates or social workers. This data-driven approach suggests that when traditional family structures are absent, the integration of professional “decision partners” and broader social networks becomes a key factor in maintaining high standards of care.
Additional Reading and References
by editor | Mar 25, 2026 | Keys to Compassionate Care
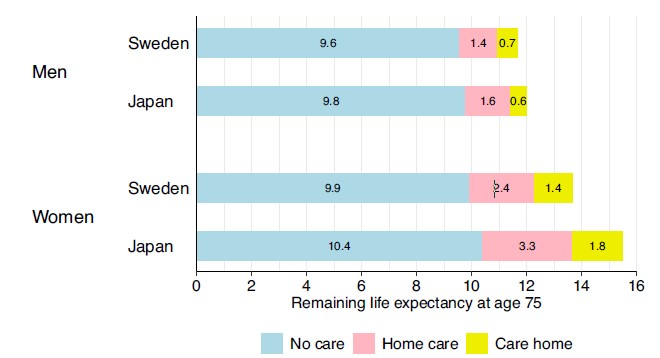
Japan has long been the global benchmark for longevity, particularly among women. Traditional explanations have often pointed to a healthy diet and specific cultural practices. However, a new study published in BMC Medicine (2026) suggests a more complex reality. By comparing the entire population over age 75 in Sweden with significant cohorts in Japan, researchers discovered that Japan’s mortality advantage is most pronounced among those already using long-term care (LTC) rather than in the healthy population.
Understanding the “Care Advantage”
The study utilized a multistate model to track transitions between independent living, home care, and care home residence. Results showed that while a 75-year-old Japanese woman can expect to live 1.8 years longer than her Swedish counterpart, more than half of that extra time – roughly 1.3 years – is spent utilizing formal long-term care services. In fact, the mortality gap widened as the level of care increased: Japanese care home residents showed significantly lower death rates than those in Sweden, with differences reaching 148 deaths per 1,000 person-years for women.
Quality of Life vs. Quantity of Years
These findings indicate that Japan’s longevity may stem less from a “healthier” population and more from extensive, high-quality medical intervention and life-sustaining treatments within the LTC system. Japan is known for some of the most intensive medical care globally. This includes high rates of doctor consultations and longer hospital stays compared to Sweden. This “care advantage” suggests that the Japanese system excels at prolonging survival even after a person has become frail or severely disabled.
The Philosophical Crossroads: Life at Any Cost?
This data brings us to a profound ethical crossroads: what is the true goal of geriatric care?
If a significant portion of added life expectancy is spent in a state of high dependency, is our medical success occasionally clashing with the patient’s quality of life. In Japan, cultural values have historically emphasized extensive end-of-life care. Yet, this raises questions about whether we are prioritizing “life extension” over the dignity and autonomy of the individual.
Dignity in the “Dependent” Years
As we look to the future of hospice and palliative care, the Japan-Sweden comparison serves as a mirror for our own values. If the secret to longevity is more intensive medicalization of the elderly, are we prepared for the social and personal costs of prolonged frailty? Should public health success be measured by the number of years we can extract from a body? Or, should success be measured by alignment of medical care with a patient’s personal preferences and their sense of well-being in their final chapters.
Bridging the Gap in Hospice Care
Ultimately, the findings suggest that strategies to extend life must be balanced with the promotion of comfort and dignity. The challenge is ensuring that “more care” does not simply mean “more intervention.” Rather, additional care should be aligned with higher quality support that honors the human experience. We must continue to advocate for a care model where longevity never comes at the expense of a peaceful and dignified end-of-life journey.
Further Reading and References
.
.
.
.

by editor | Mar 22, 2026 | Blog, Keys to Compassionate Care, Resources and Readings
The healthcare landscape is rapidly evolving, moving beyond AI as a simple administrative tool toward its potential as an “Artificial Moral Agent.” An intriguing article in the Hastings Center Report, “What Does Moral Agency Mean for Nurses in the Era of Artificial Intelligence?” (Ulrich et al., 2026), explores the shifting boundaries between human clinical judgment and advanced AI systems.
At its core, the piece examines the concept of “moral agency” – the ability to discern right from wrong and be held accountable – which has historically been a uniquely human trait. As AI begins to summarize patient conversations, predict care outcomes, and even simulate empathy, we must question whether these systems are merely sophisticated tools or if they are evolving into entities that could one day supplant the ethical responsibilities of healthcare professionals.
Sentience vs. Simulation: The Question of Accountability
The article raises profound ethical questions regarding the nature of consciousness and responsibility in machines. It highlights the debate between those who view AI as “moral zombies” – systems that lack the sentience and feelings of sympathy required for true morality – and those who argue for a functional “artificial moral responsibility.”
The text prompts us to consider if a machine can truly be held “accountable” if it lacks a self-perception of harm, or if it can ever replicate the “practical wisdom” that a human clinician develops through years of bedside experience. Interestingly, the research even touches on the “0.1% rule,” questioning at what point humans might have a moral obligation to treat AI entities with dignity if there is even a negligible chance they possess self-awareness.
Can a “Moral Zombie” Truly Value a Patient?
Furthermore, the authors explore the risk of “mindless morality,” where systems are programmed with embedded values but lack a genuine understanding of them. This raises the critical question of whether an AI can ever truly “value” a patient or if it is simply reflecting an artifact of high-speed information processing. The article avoids a definitive conclusion on whether AI can be moral. Instead, it is framed as a tension: while AI can reduce cognitive burdens and offer probabilistic insights, the “healing power of shared humanity” remains an intuitive, non-algorithmic exchange. These questions force a re-evaluation of whether moral agency is a set of logical rules to be programmed or an irreplaceable human connection rooted in our shared vulnerability.
The Near-Term Impact: AI as a Resource, Not a Partner
For clinicians working in hospice and palliative care, these insights translate into a dual reality of enhanced data and protected human presence. In the near term, hospice workers may find AI exceptionally useful for predicting staffing needs, summarizing complex patient records, or flagging subtle clinical changes. However, the research argues that the most sensitive aspects of hospice – discussions regarding end-of-life goals, the navigation of grief, and the honoring of personal dignity – must remain strictly within the human domain. Clinicians are encouraged to view AI as a “resource” rather than a “partner.” This will ensure that the final application of any AI-suggested protocol is filtered through clinicians’ own moral discernment and the specific values of the dying patient.
Long-Term Outlook: Preserving the Sacred Human Connection
In the long term, the impact on hospice care will likely focus on the preservation of “therapeutic presence.” As AI takes over administrative and even some diagnostic functions, the role of the hospice clinician may shift more heavily toward being the primary “moral agent” who speaks up when a data-driven prediction conflicts with a patient’s unique wishes. The future of hospice depends on clinicians actively shaping the “moral codes” embedded in these technologies. By doing so, they ensure that AI supports, rather than erodes, the sacred trust between those at the end of life and the professionals who see, hear, and value them as humans, not as data points.
Additional Reading and Resources
by editor | Mar 22, 2026 | Blog, Compliance and Regulatory - Directors, Keys to Compassionate Care, Regulatory Compliance
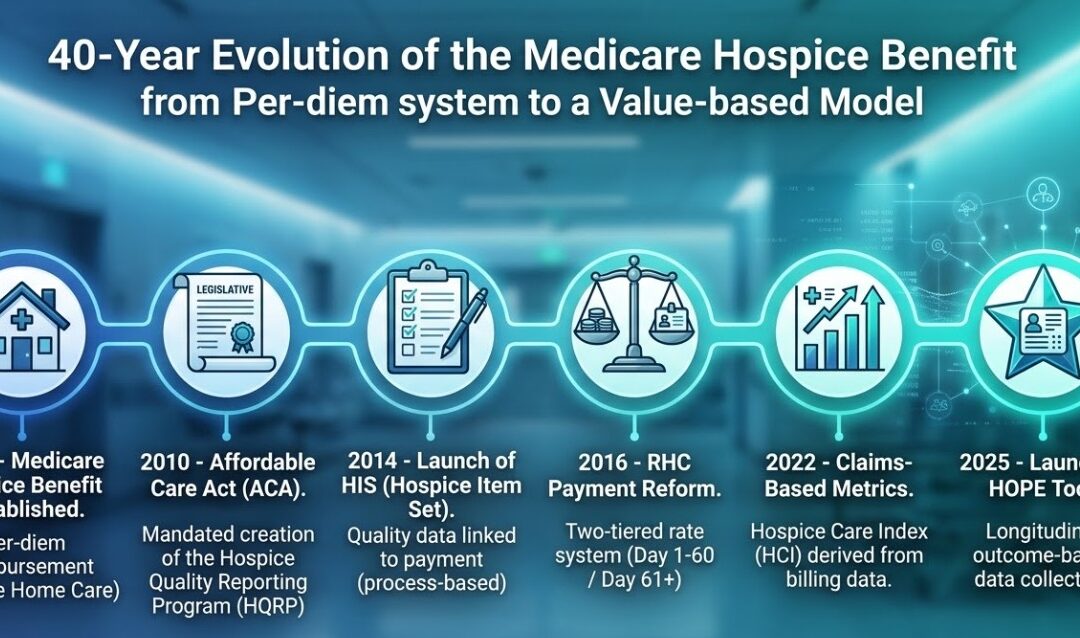
Hospice care, since its inception, has been about compassionate care. However, the underlying mechanisms of how it is paid for and how hospice quality is evaluated have undergone a significant transformation. This shift is part of a broader healthcare movement towards value-based care, moving away from simple fee-for-service models. For hospice, this journey can be understood through key eras and events.
1. The Foundation: 1983–2010
The concept of hospice care solidified with the establishment of the Medicare Hospice Benefit in 1983. This landmark legislation provided a structured way for Medicare beneficiaries to access comprehensive end-of-life care. Originally designed with a primary focus on cancer patients and shorter lengths of stay, it reflected the understanding of terminal care at the time. The reimbursement structure was a per-diem (per day) payment. This model, while straightforward, did not initially distinguish between different levels of care intensity.
The Medicare Hospice Benefit was established in 1983 under the Tax Equity and Fiscal Responsibility Act (TEFRA). For nearly three decades, the payment model was simple: a flat per-diem rate for four levels of care. It was designed for a different era – primarily for cancer patients with short, predictable lengths of stay. During this “Static Era,” CMS had financial data on what they paid, but almost no clinical data on what was actually happening in the home.
2. The Turn Toward Accountability: 2010–2014
As hospice use grew and patient demographics evolved, questions arose about varying practices and quality across providers. This ushered in an era focused on accountability and data collection. The Affordable Care Act (ACA) of 2010 changed the legal landscape. It mandated the creation of the Hospice Quality Reporting Program (HQRP). This marked a fundamental shift, transforming quality reporting from a voluntary endeavor into a mandated requirement for all hospice agencies.
A pivotal moment in this data-driven approach was the 2014 introduction of the Hospice Item Set (HIS). For the first time, agencies were required to submit standardized data on specific quality processes. This also tied hospice quality to payment. Failure to report HIS data resulted in a 2% (now 4%) reduction in the annual payment update.
However, HIS was a “process-based” tool. It measured if a hospice performed an action (like asking about pain), not whether the patient actually improved. Thus, while HIS was a vital step forward, its process-oriented nature was essentially retrospective. It confirmed whether specific admission and discharge procedures were documented, not necessarily if the patient’s well-being improved as a result.
3. Rebalancing the Payment Model: 2016
Parallel to the quality reporting initiatives, CMS implemented structural changes to the hospice payment system itself. In 2016, a significant change was introduced for Routine Home Care (RHC) payments. CMS realized the flat per-diem rate for Routine Home Care (RHC) didn’t match the reality of care delivery. This wasn’t about reducing payments, but about acknowledging the higher intensity of services typically required during the initial 60 days and the final days of a patient’s life.
CMS implemented RHC Payment Reform, creating two separate RHC rates: a higher rate for days 1–60 and a lower rate for days 61+. This was a structural signal that CMS was closely analyzing length-of-stay data and visit intensity. The different per-diem rates were were intended to incentivize a better alignment of payments with actual resource utilization.
Another key milestone was the creation of claims-based metrics. Recognizing the treasure trove of data within existing claims submissions, CMS developed indicators such as those within the Hospice Care Index (HCI). This approach utilized claims data to look for patterns related to care quality, such as the frequency of visits in the last days of life. This represents a clever use of existing data to derive quality insights, moving beyond self-reported assessments.
4. The Era of “Invisible” Metrics: 2022–Present
While agencies were focused on their clinical notes, CMS began using the bills themselves to measure quality. In 2022, they introduced the Hospice Care Index (HCI), a claims-based measure consisting of 10 indicators.
Unlike HIS, which clinicians fill out, the HCI is calculated entirely from existing claims data. This allows Medicare to identify patterns – like “live discharges” or “visits in the last days of life” – without requiring new forms, moving the industry closer to a Value-Based Purchasing mindset.
5. The Failed “Carve-In” and the Path to HOPE: 2021–2025
CMS also engaged in direct testing of value-based models through various pilots and demonstrations. One prominent example was the hospice component of the Value-Based Insurance Design (VBID) Model, often called the “hospice carve-in.” Launched in 2021, Value-Based Insurance Design (VBID) allowed Medicare Advantage plans to manage hospice benefits.
The goals of the VBID hospice carve-in were to assess if integrating hospice within a Medicare Advantage plan could improve care coordination, enhance quality, and reduce spending by preventing unnecessary hospitalizations. This initiative ran until 2024. The insights gained from this experiment, particularly regarding the need for robust quality measures and care coordination, continue to influence the overall direction of hospice payment and quality strategy. The experiment officially ended in December 2024, largely because CMS lacked a standardized, real-time clinical assessment tool to measure outcomes across different plans.
This brings us to the present. The Hospice Outcomes and Patient Evaluation (HOPE) tool, effective October 1, 2025, is the direct answer to this 40-year journey. CMS has finally reached a point where they are no longer satisfied with process checkboxes; they are building the infrastructure to pay for the actual impact of care.
The Path Forward and Why This Matters
The cumulative experiences from these various efforts – the process metrics of HIS, the structural changes in RHC payments, the deployment of claims-based metrics, and the practical learnings from models like VBID – all pointed to a persistent need. The industry required a standardized, patient-centric way to measure actual patient outcomes rather than just processes. This recognized need for more meaningful, outcome-focused data is a direct driver behind the development of the Hospice Outcomes and Patient Evaluation (HOPE) tool, that replaced HIS in late 2025. HOPE aims to capture data longitudinally during a patient’s stay, focusing on symptom impact and goal-setting – providing the rich data environment necessary to genuinely advance value-based care in hospice.
This historical overview illustrates that the shift towards value-based care in hospice is not a recent or sudden development. It has been a steady, deliberate evolution building upon the foundation laid in 1983, constantly striving for a more refined, data-driven system that ultimately ensures high-quality care is both provided and effectively measured. Every regulation, from the ACA to the HOPE tool, has been a stepping stone toward a system that rewards agencies for clinical outcomes rather than just census volume.

by editor | Mar 16, 2026 | Accounts Receivable, Billing - General, Blog, Keys to Compassionate Care
Our previous installments, Strategic Hospice Revenue Cycle Management and Hospice Billing: How to Build a Clean-Claim Process, established that a healthy revenue cycle is the engine that allows an agency to maintain stability and focus on its clinical mission. However, hospice leadership typically focus more heavily on clinical delivery rather than the financial aspects of the agency. The connection between daily administrative tasks and long-term financial health can sometimes be difficult to see.
Many leaders find that their month-end feels like a period of high volatility rather than a repeatable operating process. To shift to a more predictible financial stance, leadership must transition from merely monitoring bank balances to auditing the upstream processes that dictate the agency’s cash flow.
Hospice leadership to not need to be a billing experts to lead a successful agency. However, it is essential to have a solid understanding of the operational triggers that dictate the agency’s cash flow. To gain an understanding of the agency’s health and whether the agency is running a disciplined or reactive process, leadership can use these seven questions in the next meeting with the revenue cycle manager.
1. The “First-Pass” Health Check
The Question: “What is our first-pass clean claim rate over the last 90 days, and what are the primary reasons for failure?”
Why it matters: A “first-pass” claim is one that is paid by Medicare the very first time the agency submits it. In a healthy agency, this should be above 95%. A high first-pass rate indicates that the intake and clinical teams are providing the billing office with clean, validated data. If the first-pass rate is low, it means the billing team is spending more time “fixing” old errors than processing new revenue. A low first-pass rate means that the billing team is spending more time reworking old claims and fixing old mistakes than processing new revenue.
Leadership needs to know why claims are failing. Is it because intake forms are missing signatures? Is it because the clinical notes don’t match the billing dates? This question tells leadership which department – Intake, Clinical, or Billing – needs more training.
2. The NOE Revenue Leak
The Question: “How many non-covered days did we incur last month due to late or returned NOEs, and what was the specific dollar impact?”
Why it matters: The Notice of Election (NOE) is the most time-sensitive document in hospice. An agency has exactly five calendar days from a patient’s admission to notify Medicare. If the agency misses that window, or if the agency submits it with an error and has to resubmit it late, Medicare will simply refuse to pay for the days the agency cared for the patient prior to the NOE submission date. This is not a “delayed” payment; it is lost revenue that can never be recovered. Thus, unlike most billing errors, Notice of Election (NOE) failures typically result in permanent losses, i.e., “non-reportable” days where care was provided but cannot be reimbursed.
Tracking the dollar amount of these “non-covered days” is the fastest way to see if the agency’s intake process is disciplined. Quantifying the non-covered days in dollars transforms a “paperwork issue” into a tangible loss that requires immediate leadership intervention.
3. Sequential Discipline
The Question: “Are we experiencing out-of-sequence rejections, and if so, what is the root cause?”
Why it matters: Hospice billing is linear. Medicare processes hospice claims in a strict chronological order. An agency cannot successfully bill for a patient’s February services until the patient’s January claim has been processed and paid. This is known as sequential billing. One unclosed transfer, discharge, or revocation can halt the entire chain of claims for a patient.
Sequencing issues usually point to a breakdown in communication between field staff and the office, indicating that patient statuses are not being updated in the EMR in real-time.
If a patient’s status changes – such as a transfer from another agency, a discharge, or a readmission – the paperwork must be finalized in the system with perfect accuracy. If a single status update is forgotten or entered incorrectly, it creates a billing stoppage. Every subsequent month of revenue for that patient is held in “suspense” by Medicare until the prior month is resolved. This question reveals whether the agency’s clinical and office staff are communicating patient status changes in real-time, or if the agency’s billing department is constantly waiting on clinical data to “unlock” the next month’s cash flow.
4. The Eligibility Safety Net
The Question: “What is our 30-day forward-looking tracker for recertifications and Face-to-Face (F2F) deadlines?”
Why it matters: To keep a patient on hospice, a physician must certify their eligibility at specific intervals. For some of these, a “Face-to-Face” visit is legally required. If that visit happens even one day late, the patient’s eligibility is voided for that period, and the claim will be denied. These are unnecessary and preventable revenue lossses.
Hospice leadership should ensure that the team isn’t just reacting to missed deadlines. Instead, the team should be actively managing a calendar of upcoming recertification requirements – proactively tracking patients with upcoming recertifications – to ensure no patient “falls out of compliance.”
5. “Return to Provider” (RTP) Velocity
The Question: “What is our average ‘Time to Correct’ for claims that are Returned to Provider (RTP)?”
Why it matters: Claims are often returned for small technical errors (like a misspelled name or an incorrect ZIP code). While the error might be minor, the impact on cash flow is major. If it takes the billing team five days to notice and fix an error, the agency has effectively added five days to its “Days in AR” (the time it takes to get paid). To keep cash moving, high-performing teams aim to correct and resubmit RTPs within 24–48 hours. A high “time to correct” often indicates that the billing team lacks the necessary support from clinical leadership to resolve documentation gaps.
6. Handoff Accountability
The Question: “If you could fix one upstream process – Intake, Clinical, or Medical Director workflows – to reduce rework, which would it be?”
Why it matters: The answer to this important question gives significant insight into where “administrative friction” can be slowing down a hospice agency’s money. Billing managers often see the “symptoms” of problems that start elsewhere. For example, if the billing manager says they spend hours chasing doctors for signatures, the problem isn’t the billing – it’s the physician’s workflow.
This question breaks down operational silos. It gives the revenue cycle manager permission to identify where “dirty data” originates. Often, a minor adjustment to an admission packet or how a Medical Director receives prompts can eliminate 50% of the billing team’s manual labor.
7. The Close Process
The Question: “What is our documented ‘Month-End Close’ checklist and who owns the accountability for each handoff?”
Why it matters: The “Month-End Close” is the process of finalizing all clinical and financial data so the bills can go out. If clinical notes aren’t finished on time, the biller can’t bill. If the biller is waiting on the director to approve a report, the biller can’t bill. A clear, written checklist ensures that everyone knows their role and how it contributes to the agency’s overall ability to bill on time. Hospice leadership owns the accountability for ensuring that the clinical staff doesn’t treat documentation as an “optional” task; such an approach to documentation can delay the entire agency’s payroll and vendor payments.
When the month-end process is a mystery to everyone but the billing team, the result is process uncertainty and cash flow volatility. A disciplined system relies on a written checklist that defines when clinical notes are due, when statuses must be closed, and when the pre-bill review occurs. Accountability ensures the billing team isn’t held responsible for a clinical manager’s late paperwork.
Why This Matters for Hospice Leadership
By moving from a “scramble” to a “system,” hospice leadership protects the agency’s ability to serve patients. When the revenue cycle is predictable, leadership can stop worrying about whether payroll can be met and can start focusing on the quality of the end-of-life care that the team provides.
